Last week, Florida's Governor Ron DeSantis convened a panel of 'experts' to try and prove mRNA vaccines are unsafe.
We wanted to point out some key myths which illustrate how they continue to mislead people. 🧵
We wanted to point out some key myths which illustrate how they continue to mislead people. 🧵

Many of their claims center around distorting the real side-effect of myocarditis. The first is this narrative that history has shown that this side effect is riskier for kids than the virus.
We *know* this is false. AAP data show most kids 12-17 were fully vaccinated by August.
We *know* this is false. AAP data show most kids 12-17 were fully vaccinated by August.

At this point, national data showed only 543 confirmed cases of vaccine-associated myocarditis in kids. And since 0-11 year olds are at very low risk for this event, there would be a limit to its scale.
Contrast this with 170000+ reported pediatric hospitalizations from COVID.
Contrast this with 170000+ reported pediatric hospitalizations from COVID.

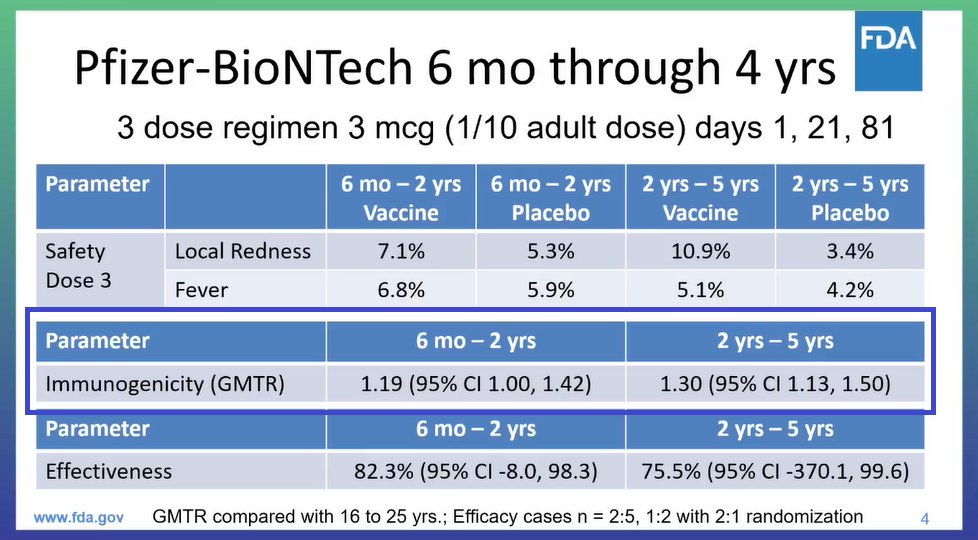
Another set of myths involves looking at the original clinical trials to determine if vaccines "really work."
This makes no sense because (in the US) we intentionally limited harms from COVID in the trial. The reason being so that the placebo group could get the vaccine...
This makes no sense because (in the US) we intentionally limited harms from COVID in the trial. The reason being so that the placebo group could get the vaccine...
When you look at real-world data for hundreds of thousands of ppl—matched by age, gender and class—you find all of the most significant outcomes are FAR worse with COVID.
This is better than cherry picking small trials designed not to let people get hurt. nejm.org/doi/10.1056/NE…
This is better than cherry picking small trials designed not to let people get hurt. nejm.org/doi/10.1056/NE…

Panelist Joseph Ladapo then tries to claim that vaccine harms go unreported because: "These people are dying before they get to the hospital."
That's categorically false. Studies using electronic data on outcomes (instead of voluntary reports) find no increase in arrhythmia.
That's categorically false. Studies using electronic data on outcomes (instead of voluntary reports) find no increase in arrhythmia.

Ladapo also tries to claim that autopsies show vaccine associated sudden cardiac death.
His only proof is a case report with four older patients who died of arrhythmia. While they did have subclinical myocarditis, they also had pre-existing heart disease.
His only proof is a case report with four older patients who died of arrhythmia. While they did have subclinical myocarditis, they also had pre-existing heart disease.
https://twitter.com/han_francis/status/1599772912906514434?s=20&t=pXQAj7BiimMVY7AE3pkc6g
Given arrhythmias are the #1 natural cause of death it's a jump to say vaccines caused this.
In fact, a Nature study following 17 million doses showed the Pfizer vaccine did NOT cause arrhythmias.
COVID, however, increased the risk three to five fold. nature.com/articles/s4159…
In fact, a Nature study following 17 million doses showed the Pfizer vaccine did NOT cause arrhythmias.
COVID, however, increased the risk three to five fold. nature.com/articles/s4159…
This study did show a slight increase following Moderna's vaccine (with a much smaller sample), but this was based on 48 events and the confidence interval included no increase in risk. So the evidence is insufficient.
Meaning—at worst—Ladapo should just opt to recommend Pfizer.
Meaning—at worst—Ladapo should just opt to recommend Pfizer.
Instead, he claims that the COVID vaccine has been shown to increase "cardiac mortality" in young men.
This isn't true. In fact, we've followed these rumors for a long time and it's hard to find any clear cut cases in the US where vaccine myocarditis was fatal...
This isn't true. In fact, we've followed these rumors for a long time and it's hard to find any clear cut cases in the US where vaccine myocarditis was fatal...

That's not to say it hasn't ever happened (we examine some edge cases in the article below), only that if it does it's exceedingly rare.
Nonetheless, Florida's government promised to uncover some hidden harms and will keep pushing this narrative...
voicesforvaccines.org/covid-vaccines…
Nonetheless, Florida's government promised to uncover some hidden harms and will keep pushing this narrative...
voicesforvaccines.org/covid-vaccines…
Well: We've been open-book about this all along, even interviewing doctors who treat both COVID and the vaccine myocarditis.
We'll tell you if some evidence proves otherwise, but right now the data clearly say that vaccination is the right choice.
#GetVaccinated 🩹
We'll tell you if some evidence proves otherwise, but right now the data clearly say that vaccination is the right choice.
#GetVaccinated 🩹
For broader perspective, Florida's Health Department got the data on kid's vaccines wrong nine months ago.
We've addressed their claims before even if they want you to think no one is talking about them.
We've addressed their claims before even if they want you to think no one is talking about them.
https://twitter.com/Voices4Vaccines/status/1504101211221417985?s=20&t=wQYLIO-azT-ykUlOnaLTfg
• • •
Missing some Tweet in this thread? You can try to
force a refresh