Familiar?
Expert opinions misaligned with CDC & its low & no evidence guidelines are deemed “false information” by those who run simulations in the public consciousness via social & legacy media.
Public health has maimed & killed for nearly a century with no accountability. 🧵
Expert opinions misaligned with CDC & its low & no evidence guidelines are deemed “false information” by those who run simulations in the public consciousness via social & legacy media.
Public health has maimed & killed for nearly a century with no accountability. 🧵
https://twitter.com/davidzweig/status/1607386849772716037
Everyone has likely heard of the Tuskegee Study. A whitewashed name for what was once known, according to CDC, as the “Tuskegee Study of Untreated Syphilis in the Negro Male.”
It began in 1932 under the management of the federal United States Public Health Service (USPHS or PHS)
It began in 1932 under the management of the federal United States Public Health Service (USPHS or PHS)
The study targeted black men & focused on recording “the natural history of syphilis,” a chronic, contagious bacterial infection that can be venereal or sometimes, congenital.
15-30% of people infected who don't get treatment will develop complications known as tertiary syphilis
15-30% of people infected who don't get treatment will develop complications known as tertiary syphilis

The purpose of the study was to observe the UNTREATED (“natural”) course of the disease until death, which included autopsy findings.
Some facts about the study:
• It involved 600 black men
• 399 had syphilis
• 201 did not have the disease
Some facts about the study:
• It involved 600 black men
• 399 had syphilis
• 201 did not have the disease
Continued:
• The men were told they were being TREATED for “bad blood” a term used to describe several ailments, including anemia and fatigue
• The men received free medical exams, meals, and burial insurance in exchange for taking part in the study
cdc.gov/tuskegee/timel…
• The men were told they were being TREATED for “bad blood” a term used to describe several ailments, including anemia and fatigue
• The men received free medical exams, meals, and burial insurance in exchange for taking part in the study
cdc.gov/tuskegee/timel…
A few distinctive features of this highly unethical experiment:
• Informed consent was neither sought nor obtained
• By 1942, Penicillin was available
• By 1943, 11 years after the study commenced, Penicillin is a KNOWN CURE and becomes treatment of choice for the disease
• Informed consent was neither sought nor obtained
• By 1942, Penicillin was available
• By 1943, 11 years after the study commenced, Penicillin is a KNOWN CURE and becomes treatment of choice for the disease

Continued:
• “Treatment was withheld from more than half of them, even after penicillin was discovered as a cure for the disease.”
USA Today claims CDC “wasn’t involved” even though they were “complicit.” 🧐
usatoday.com/story/news/fac…
• “Treatment was withheld from more than half of them, even after penicillin was discovered as a cure for the disease.”
USA Today claims CDC “wasn’t involved” even though they were “complicit.” 🧐
usatoday.com/story/news/fac…
Continued:
• In 1972 the first news article exposing the study is published by Jean Heller at The Associated Press
• The study ends on the recommendation of an Ad Hoc Advisory Panel convened by the Assistant Secretary for Health and Scientific Affairs
• In 1972 the first news article exposing the study is published by Jean Heller at The Associated Press
• The study ends on the recommendation of an Ad Hoc Advisory Panel convened by the Assistant Secretary for Health and Scientific Affairs

Continued:
• 1997 President Clinton issues a formal Presidential apology
• In 2004, the last participant dies
• In 2009, the last widow of a participant dies
What does any of this have to do with the CDC?
• 1997 President Clinton issues a formal Presidential apology
• In 2004, the last participant dies
• In 2009, the last widow of a participant dies
What does any of this have to do with the CDC?
CDC was initially the “Communicable Disease Center” and was established by the USPHS in 1946, the same corrupt agency that initiated the unethical Tuskegee Study.
Officials at CDC knew about it and refused to stop it, even after a concerned doctor brought it to their attention.
Officials at CDC knew about it and refused to stop it, even after a concerned doctor brought it to their attention.
CDC maintained that consent was obtained & that the men were told they could seek treatment.
Neither claim was true.
CDC maintained this until the story broke in the press. They now host a history of the study on their website.
See excerpt from:
faculty.cbu.ca/sstewart/nurs3…
Neither claim was true.
CDC maintained this until the story broke in the press. They now host a history of the study on their website.
See excerpt from:
faculty.cbu.ca/sstewart/nurs3…

Not one of the doctors, nurses, officials who knew about, participated in, or CDC doctors who participated in or were alerted to the unethical nature of the study by Buxtun, were ever held accountable.
Fast forward to the 2010s & the disabled become a federal target.
NASEM, a collection of non-governmental organizations (NGOs), & federal agencies begin planning how to disrupt access to life saving pharmaceuticals for people with severe injury/illness across the country.
NASEM, a collection of non-governmental organizations (NGOs), & federal agencies begin planning how to disrupt access to life saving pharmaceuticals for people with severe injury/illness across the country.
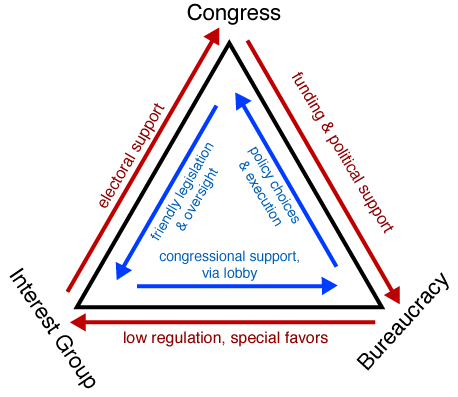
The Institute of Medicine (IOM), now the NAM, called for CDC to develop prescribing “guidelines” for pain in their 2011 report titled “Living Well with Chronic Illness.”
CDC does this with the help of special interest group “Physicians for Responsible Opioid Prescribing” (PROP).
CDC does this with the help of special interest group “Physicians for Responsible Opioid Prescribing” (PROP).
PROP is an extreme anti-opioid interest group founded by Andrew Kolodny, an addiction specialist who doesn’t treat pain, or the myriad chronic illnesses and injuries that cause it.
2015, CDC holds a private meeting with PROP members titled the Core Expert Group (CEG).
2015, CDC holds a private meeting with PROP members titled the Core Expert Group (CEG).
This meeting of mostly addiction “experts” discussed the development of CDC’s prescribing guidelines for chronic pain and how they’d be structured.
A guideline that would end up creating barriers to care for sick & injured people. We didn’t know the extent of the discussion, …
A guideline that would end up creating barriers to care for sick & injured people. We didn’t know the extent of the discussion, …
what “experts” were present, or what conflicts of interest (COIs) they may have had, because CDC & HHS made use of 2 exemptions that allowed the redaction of nearly every word in documents requested under FOIA.
Names leaked anyway & COIs later declared.
painnewsnetwork.org/stories/2020/4…
Names leaked anyway & COIs later declared.
painnewsnetwork.org/stories/2020/4…
This is the letter CDC sent to the Editor of PNN after they requested documents pertaining to the secretive 2015 CEG meeting.
static1.squarespace.com/static/54d50ce…
These same exemptions (5 U.S.C. §552 Exemptions (b)(5) and (b)(6) were later cited in government documents related to COVID-19.
static1.squarespace.com/static/54d50ce…
These same exemptions (5 U.S.C. §552 Exemptions (b)(5) and (b)(6) were later cited in government documents related to COVID-19.
In 2016, the CDC’s guidelines on prescribing are published and the Drug Enforcement Agency (DEA) ramps up efforts to arrest/prosecute physicians who are prescribing outside of CDC’s “voluntary” recommendations.
DEA gets much funding via civil asset forfeiture-Perverse incentive.
DEA gets much funding via civil asset forfeiture-Perverse incentive.
The newly released “voluntary guidelines” result in physicians across the country forcing their patients off of opioids, including cancer patients while those working with hospice patients are scared to initiate pain control for end of life care over fears of “addiction.”
Many, including veterans, begin committing suicide or die from complications of rapid forced tapers which often lasted only 1 day.
The VA knew pain intensity was correlated to suicide attempts but continued force tapering vets anyway.
news.va.gov/67708/va-study…
The VA knew pain intensity was correlated to suicide attempts but continued force tapering vets anyway.
news.va.gov/67708/va-study…
The “opioid crisis” was a pilot for engineered health crises that taught public health agencies how to misdirect the public, stigmatize patients & ensure compliance with future public health mandates & policies by running taxpayer funded media campaigns discrediting dissidents …
& justifying government overreach. HHS then establishes the IPRCC as part of the ACA to coordinate all pain research within HHS & across federal agencies.
In 2017, the Federal Pain Research Strategy (FPRS) is published which outlined how pain research would be conducted by NIH.
In 2017, the Federal Pain Research Strategy (FPRS) is published which outlined how pain research would be conducted by NIH.
Many of NIH’s embedded Pragmatic Clinical Trials (ePCTs) are done w/out patient knowledge or consent. This research at the bedside, critics say, is widespread government experimentation on untreated patients in pain.
No outcomes studies have ever been conducted by government.
No outcomes studies have ever been conducted by government.
CDC ensured terrified doctors forced patients off drugs providing quality of life. NIH had more research subjects to study non-opioid treatments, which are often more expensive & less effective.
Many affected by these & other public health policies are dead. No accountability.
Many affected by these & other public health policies are dead. No accountability.
CDC’s own data shows that as dispensing has decreased, overdose deaths have increased.
This is because prescription analgesics were keeping many who require medical management of pain (and even other users) away from much more dangerous illicit supplies with unknown potency.
This is because prescription analgesics were keeping many who require medical management of pain (and even other users) away from much more dangerous illicit supplies with unknown potency.


The problem of dangerous drugs has been compounded by several orders of magnitude since HHS & CDC involved themselves. Illicit drugs are ⏩ volatile than ever with ⏩ death than ever.
These public health policies exacerbated one crisis & ensured the creation of a whole new one.
These public health policies exacerbated one crisis & ensured the creation of a whole new one.
How long are we expected to fund what seems to be intentional failure by PH agencies to protect health while our tax $ are used to mercilessly manipulate, maim & torture us? How long should we accept epistemic violence (violence exerted against or through knowledge) as normative?
We still don’t know how many of the patients affected by the CDC’s 2016 guidelines have died.
There have been no outcomes studies conducted by any of these agencies, even after the FDA, HHS, and CDC published warnings against rapid forced tapers.
We’ll likely never know.
There have been no outcomes studies conducted by any of these agencies, even after the FDA, HHS, and CDC published warnings against rapid forced tapers.
We’ll likely never know.
To learn more about the plight of patients who’ve been swept up in the #WarOnDrugs, see my draft report, a 20-year overview of drug-related statistics.
Download the report via SSRN. It contains several hundred graphs depicting government drug data.
papers.ssrn.com/sol3/papers.cf…
Download the report via SSRN. It contains several hundred graphs depicting government drug data.
papers.ssrn.com/sol3/papers.cf…
Final note:
CDC accomplished this by pushing MISLEADING statistics on the public, which in essence, manufactured their consent for draconian policies.
The war on drugs now includes patients & their doctors thanks to taxpayer funded CDC media campaigns.
medium.com/the-shadow/scr…
CDC accomplished this by pushing MISLEADING statistics on the public, which in essence, manufactured their consent for draconian policies.
The war on drugs now includes patients & their doctors thanks to taxpayer funded CDC media campaigns.
medium.com/the-shadow/scr…
CDC still hasn’t released info on how much taxpayer $$$ was spent in efforts to stigmatize patients, manufacture consent for policies no pain management specialists supported, & resulted in a litigation narrative that only helped lawyers & made “experts” rich while patients died.
@EthicalSkeptic, please consider researching & commenting on how CDC, other public health agencies, & NGO’s destroyed legal/medical access to analgesics.
Selective “evidence” & misleading statistics aligning with a political agenda were used to justify imposing barriers to care.
Selective “evidence” & misleading statistics aligning with a political agenda were used to justify imposing barriers to care.
• • •
Missing some Tweet in this thread? You can try to
force a refresh