
Tomorrow is NYE, there will be partying, pills, and powders. Some leading to overdose.
I work in the ER NYE/NYD & expect a few "OD's" from said pills n powders. What exactly is in them?
A 🧵from Camden, a VERY human 28 y.o male, on the illicit drug supply
#MedED #FOAMed
I work in the ER NYE/NYD & expect a few "OD's" from said pills n powders. What exactly is in them?
A 🧵from Camden, a VERY human 28 y.o male, on the illicit drug supply
#MedED #FOAMed

Cam was out with his friends celebrating NYE with some beverages when one of his friends offered him a tan powder. Cam was pretty hesitant at first but..


Eventually peer pressure won. Cam gave it a try.
A few minutes after trying the substance...
A few minutes after trying the substance...


He started to feel groggy/lethargic, his pupils became smaller, he laid down (and I guess took of his shirt at some point) and appeared to fall asleep. He soon became completely unresponsive to belly rub and appeared to have apnea and cyanosis.



His friends panicked, they couldn't wake him up.
One friend asked "What did you give him man?"
So our first question, what substance did Cam most likely ingest?
One friend asked "What did you give him man?"
So our first question, what substance did Cam most likely ingest?
Well common things being common, lets look at the stats.
Top 3 drug overdose deaths
3⃣ Cocaine
2⃣Meth
.
.
.
.
🥇Far and away the winner, synthetic opioids. And look at that, Cam's symptoms match an opioid.
Top 3 drug overdose deaths
3⃣ Cocaine
2⃣Meth
.
.
.
.
🥇Far and away the winner, synthetic opioids. And look at that, Cam's symptoms match an opioid.

For those guessing oxycodone or even heroin. We are now in the 4th wave of the "opioid epidemic". Natural and semisynthetic opioid deaths are declining while deaths from synthetic opioids AND stimulants (alone and in combination) are rising.

Back to our friend who was asked "What did you give him man?"
He responds "a friend gave it to me and said it was a crushed M30!"
He responds "a friend gave it to me and said it was a crushed M30!"
Pictured below are "M30's". Counterfeit ("pressed") fentanyl tablets designed to look like oxy 30's.
Rainbow fent is included here. If you haven't seen them yet, you will. These are a rising cause of OD but sadly not the only pressed fent tablets.
Rainbow fent is included here. If you haven't seen them yet, you will. These are a rising cause of OD but sadly not the only pressed fent tablets.



In fact counterfeit fentanyl tablets are a HUGE problem right now. They are marketed as opioids, benzodiazepines, ADHD meds and more.
Another place they're found is peoples bodies at the medical examiner. These "pressed" pills killed Mac Miller, Prince, and uncountable others
Another place they're found is peoples bodies at the medical examiner. These "pressed" pills killed Mac Miller, Prince, and uncountable others


Just how much fentanyl is in these counterfeit tablets?
It varies. A DEA Analysis of seized fentanyl tablets found the average strength ~1.7 mg
One study of 18 counterfeit "norco" found a range of 0.6-6.6 mg,
10 fold differences within the same supply=high risk for OD
It varies. A DEA Analysis of seized fentanyl tablets found the average strength ~1.7 mg
One study of 18 counterfeit "norco" found a range of 0.6-6.6 mg,
10 fold differences within the same supply=high risk for OD


Its not just fentanyl either, fentanyl is the MOST prevalent synthetic but fentanyl/non-fentanyl opioid analogues frequently pop up in the market.
A 2021 analysis confiscated fent found only 90% fent. The 2nd most common was p-fluorofentanyl
A 2021 analysis confiscated fent found only 90% fent. The 2nd most common was p-fluorofentanyl

A medical surveillance group known as the "Toxic investigator Consortium" who sends discarded biologic samples from ED overdose patients to @CFSRE_ to screen for novel psychoactive substances found high rates of p-fluorofentanyl.
So its in products and your patients.
So its in products and your patients.

p-Flourofent is a fent analog that was popular in the 1980's under the name "China White".
It may be more potent than fentanyl and is making a bit of a resurgence now. Some speculate it is due a fentanyl precursor (4-ANPP) being scheduled but flouro-4ANPP remaining available.
It may be more potent than fentanyl and is making a bit of a resurgence now. Some speculate it is due a fentanyl precursor (4-ANPP) being scheduled but flouro-4ANPP remaining available.

What about the non fenatnyl opioids?
Introducing "Benzimidazole/Nitazene" opioids.
Many showed up in 2019 as unscheduled research chems. Some may have heard of "Iso" or isotonitazene.
Potency varies, 50 x less to 20 x more potent than fentanyl (e.g., etonitazene) in vitro
Introducing "Benzimidazole/Nitazene" opioids.
Many showed up in 2019 as unscheduled research chems. Some may have heard of "Iso" or isotonitazene.
Potency varies, 50 x less to 20 x more potent than fentanyl (e.g., etonitazene) in vitro


But opioids are opioids right? We can treat these all with naloxone.
Recognizing that Cam was experiencing a classic Opioid toxidrome, a bystander trained in naloxone admin came by and gave Cam a dose.
He started breathing more Yet he remained somewhat unresponsive
Recognizing that Cam was experiencing a classic Opioid toxidrome, a bystander trained in naloxone admin came by and gave Cam a dose.
He started breathing more Yet he remained somewhat unresponsive


What non-opioids are in the opioid supply? Well lots, but one of increasing concern is Xylazine. A veterinary alpha-2 agonist (similar to clonidine).
The group that looks at discarded blood samples in OD patients found xylazine prevalence as high as 20%. Its likely higher now.
The group that looks at discarded blood samples in OD patients found xylazine prevalence as high as 20%. Its likely higher now.

This stuff is endemic in the northeast but you can still see it in other parts of the U.S., especially Midwest/south.
It causes lots of issues and we are not sure how its impacting OD management.
In theory high dose naloxone works for other alpha-2-agonist (clonidine).
It causes lots of issues and we are not sure how its impacting OD management.
In theory high dose naloxone works for other alpha-2-agonist (clonidine).


Fearing for his safety, Camden's friends RUSH him to the emergency department.

The ED team begins treating Camden.
He is initially minimally responsive but the team gives another 2 mg of naloxone x 2 IV and he begins waking up. 🏆🙌
Wanting to get an idea of what Camden may have taken, someone eagerly orders a urine drug screen.
He is initially minimally responsive but the team gives another 2 mg of naloxone x 2 IV and he begins waking up. 🏆🙌
Wanting to get an idea of what Camden may have taken, someone eagerly orders a urine drug screen.


"RYAN WHO SENDS A URINE DRUG SCREEN THAT HAS FALSE POSITIVES, FALSE NEGATIVES, AND DOESNT REPRESENT ACUTE USE?!" You angrily shout at me.
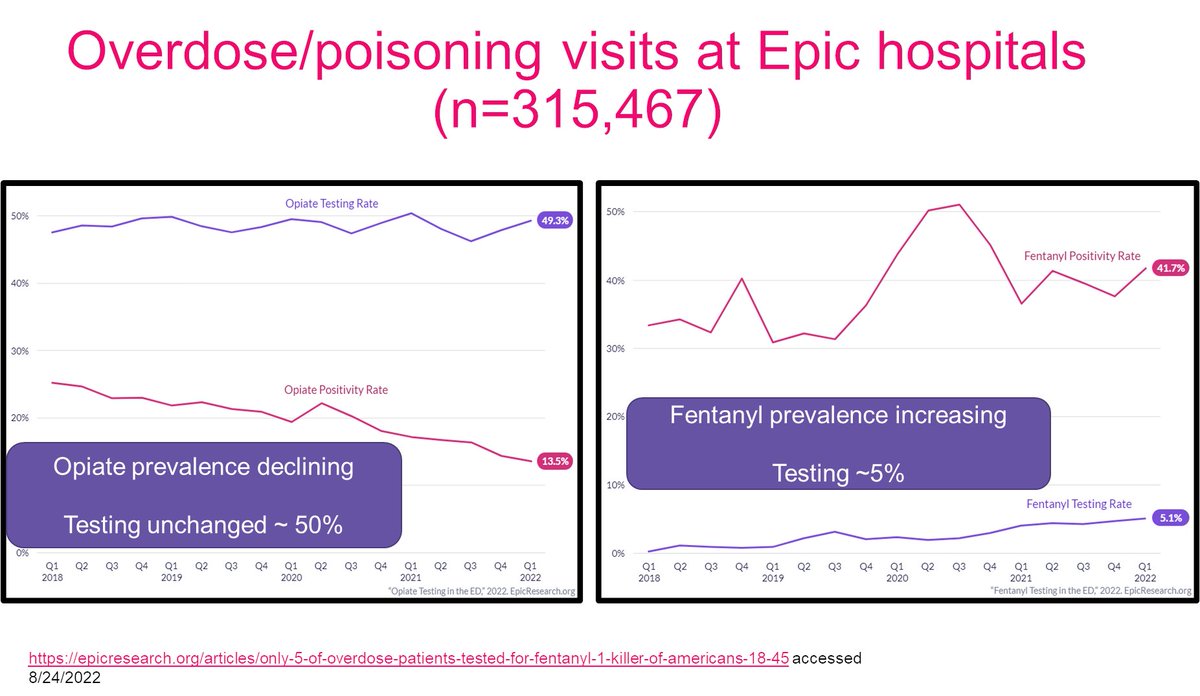
Well according to EPIC data, 50% of people treating overdoses.
Well according to EPIC data, 50% of people treating overdoses.

Sadly UDS often looks for opiates/semisynthetics.
Despite declining prevalence, testing is unchanged
Fentanyl prevalence predominates but testing for fentanyl in acute OD is dismally low.
If bother to look (thats a whole other philosophical discussion), look for fentanyl
Despite declining prevalence, testing is unchanged
Fentanyl prevalence predominates but testing for fentanyl in acute OD is dismally low.
If bother to look (thats a whole other philosophical discussion), look for fentanyl
A urinary fent is added AND....its negative
Non fentanyl opioids like nitazenes are not detectable. Other fentalogs are also prevalent, and may go undetected by commercial assay.
In one study, CARFENTANIL, the thing that tranqs polar bears, was undetected by >80% of assays
Non fentanyl opioids like nitazenes are not detectable. Other fentalogs are also prevalent, and may go undetected by commercial assay.
In one study, CARFENTANIL, the thing that tranqs polar bears, was undetected by >80% of assays

Cam is observed for several hours, a poison center is called, he gets a pysch eval and is discharged home with naloxone.
We never actually find out what Cam took. Was it an M30, ISO, p-flouro, was there xyalazine? We may never know. The landscape is ever changing
We never actually find out what Cam took. Was it an M30, ISO, p-flouro, was there xyalazine? We may never know. The landscape is ever changing

What we do know.
1. Opioids are 🥇OD death
2. Synthetics (mainly fentanyl) 🥇opioid, pressed tablets=concerning trend
3. Negative tests don't r/o exposure
4. Xylazine/p-fluoro increasing
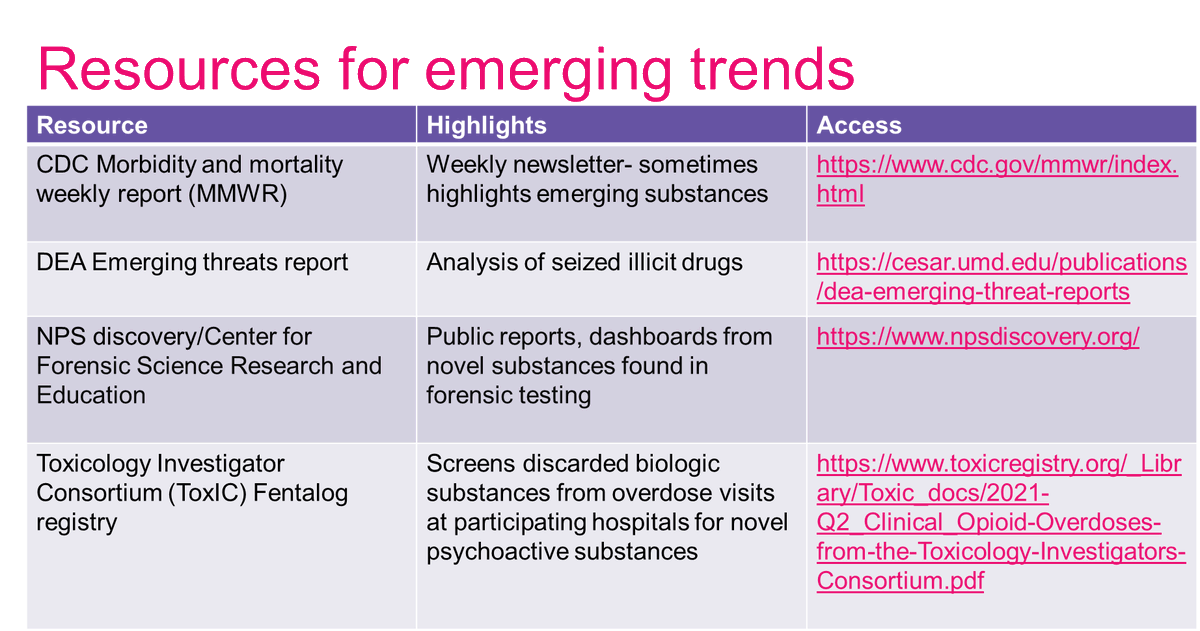
5. Landscape=changing (see table for resources)
6. Cam is a good boy
#FOAMcc #TwitteRx
1. Opioids are 🥇OD death
2. Synthetics (mainly fentanyl) 🥇opioid, pressed tablets=concerning trend
3. Negative tests don't r/o exposure
4. Xylazine/p-fluoro increasing
5. Landscape=changing (see table for resources)
6. Cam is a good boy
#FOAMcc #TwitteRx
Thanks for following along. Much of this adapted from a recent #ASHP22 presentation which some may have seen😁
If you found this useful please RT 1st tweet to spread the word on the illicit opioid supply landscape!
#harmreduction, #NYE, #Fentanyl, #Cam
If you found this useful please RT 1st tweet to spread the word on the illicit opioid supply landscape!
#harmreduction, #NYE, #Fentanyl, #Cam
https://twitter.com/EMPoisonPharmD/status/1608991915743285248?s=20&t=cU1y0QirFzYrTg0ALznUqQ
@threadreaderapp unroll
• • •
Missing some Tweet in this thread? You can try to
force a refresh











