Going to attempt a twitter space tomorrow with some cardiologists at noon to discuss a non-COVID cardiology topic.
#twitterheartspaces
We'll be discussing re-analysis of the data used to approve a common injectable medicine to lower cholesterol levels -- Evolucumab
#twitterheartspaces
We'll be discussing re-analysis of the data used to approve a common injectable medicine to lower cholesterol levels -- Evolucumab
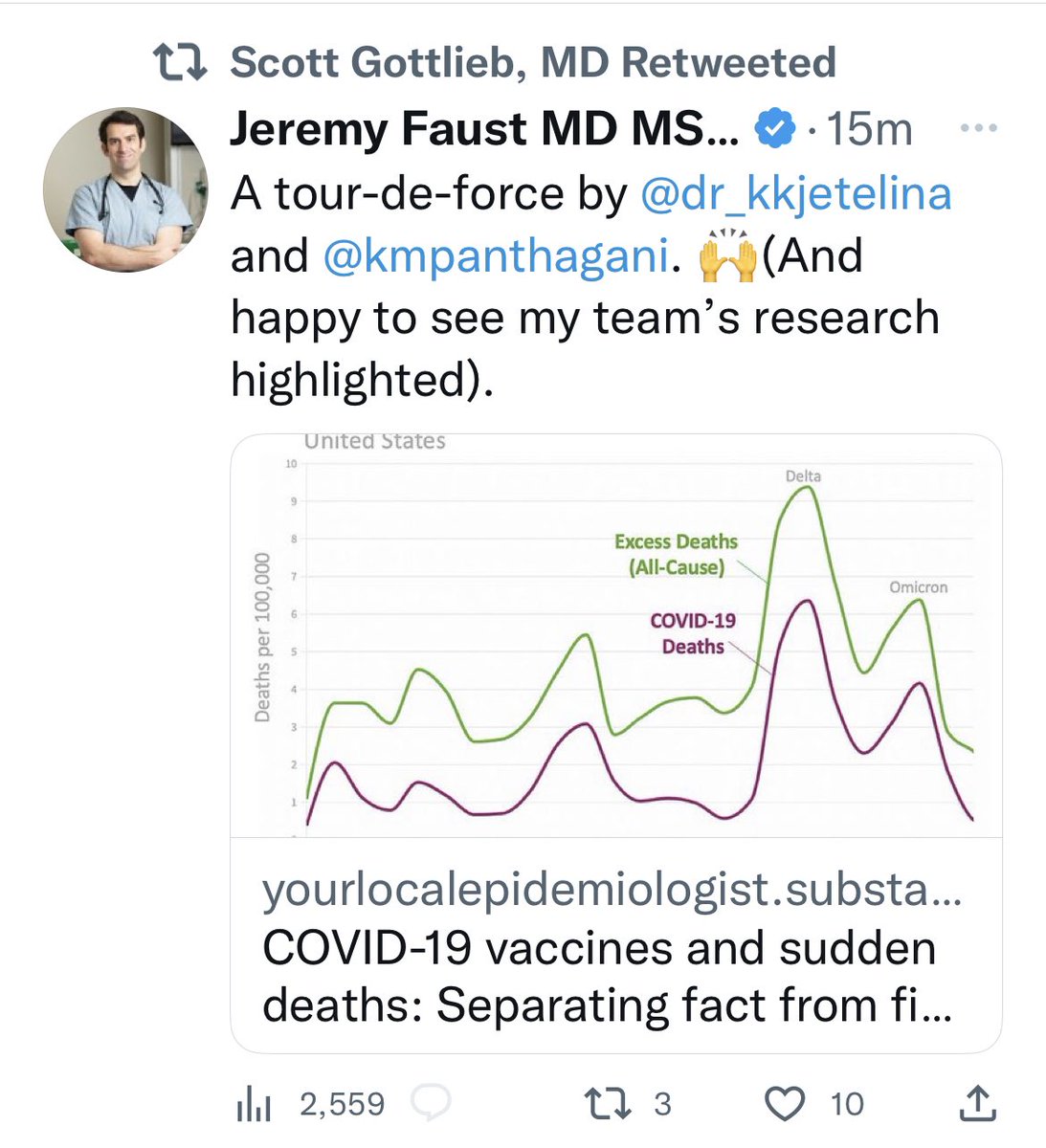
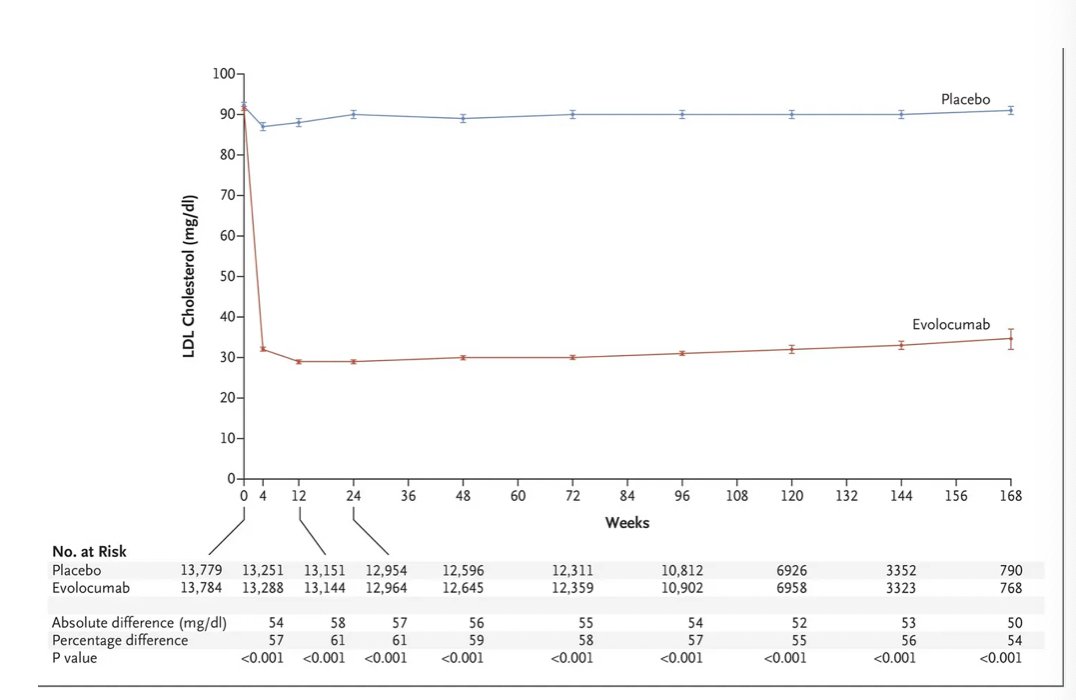
Evolucumab was shown to markedly lower LDL in patients who already had very low LDL levels to begin with.
The real question is whether it also lowered an endpoint that matters to patients like fewer heart attacks, fewer stents, or dying less..
The real question is whether it also lowered an endpoint that matters to patients like fewer heart attacks, fewer stents, or dying less..
The FOURIER primary endpoint was a composite of : (cardiovascular death, MI, stroke, unstable angina, or need for a stent/bypass) and reduced this endpoint by 1.5% (1344/13784 in the evolocumab arm vs 1563/13780 in the placebo arm)
This lead to FDA approval..
This lead to FDA approval..
This was driven almost entirely by myocardial infarction / need for revascularization . There was no difference in cardiovascular death, death from any cause.

A separate group of investigators acquired the 30,000 pages of documents submitted by the drug maker to re-analyze how the deaths in the original trial were adjudicated.. and note deaths of cardiac origin were actually higher in patients given evolocumab
bmjopen.bmj.com/content/12/12/…
bmjopen.bmj.com/content/12/12/…
The FOURIER study authors responded shortly after to note the reanalysis is fundamentally flawed because the authors did not have access to clinical source documents..
bmjopen.bmj.com/content/12/12/…
bmjopen.bmj.com/content/12/12/…
@drjohnm wrote about it for @sensible_med here..
sensiblemed.substack.com/p/yet-another-…
What does this mean for patients eligible for these injectable medications to reduce cholesterol levels ?
Listen in tomorrow !
sensiblemed.substack.com/p/yet-another-…
What does this mean for patients eligible for these injectable medications to reduce cholesterol levels ?
Listen in tomorrow !
• • •
Missing some Tweet in this thread? You can try to
force a refresh