#TREATME
Check out the charts for #longCOVID & #MECFS to see how enzymes like NK stacked up against aspirin, Plavix, DOACs (example: apixaban), and heparin. I won't do a deep dive until I gather more data & close the survey but wanted to share some data so far!🧵
Check out the charts for #longCOVID & #MECFS to see how enzymes like NK stacked up against aspirin, Plavix, DOACs (example: apixaban), and heparin. I won't do a deep dive until I gather more data & close the survey but wanted to share some data so far!🧵


Very Quick thoughts:
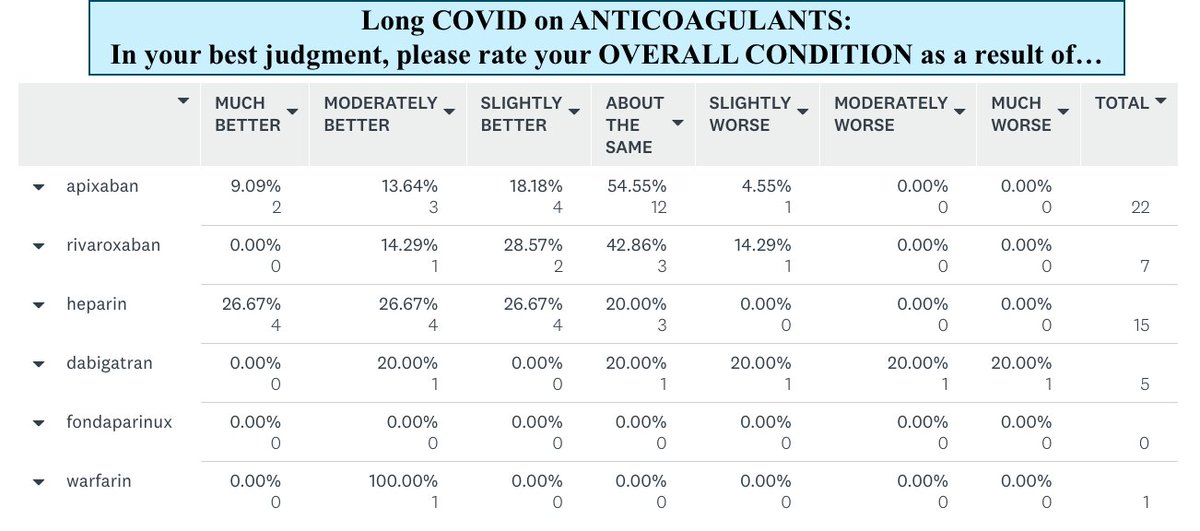
1) Oral anticoagulants alone looks subpar in #pwLC likely bc they only prevent clot formation & don't degrade existing microclots. Goal is to give body a break so it may clear clots on its own, but some may be too sick to achieve this.
1) Oral anticoagulants alone looks subpar in #pwLC likely bc they only prevent clot formation & don't degrade existing microclots. Goal is to give body a break so it may clear clots on its own, but some may be too sick to achieve this.
1) cont..
Also note small sample size, so can't draw strong conclusions yet.
2) Many #pwLC may have hyperactivated platelets so it would stand to reason than antiplatelet meds would help. While just 38% reported aspirin ALONE helped, 60% benefited from dual antiplatelet therapy.
Also note small sample size, so can't draw strong conclusions yet.
2) Many #pwLC may have hyperactivated platelets so it would stand to reason than antiplatelet meds would help. While just 38% reported aspirin ALONE helped, 60% benefited from dual antiplatelet therapy.
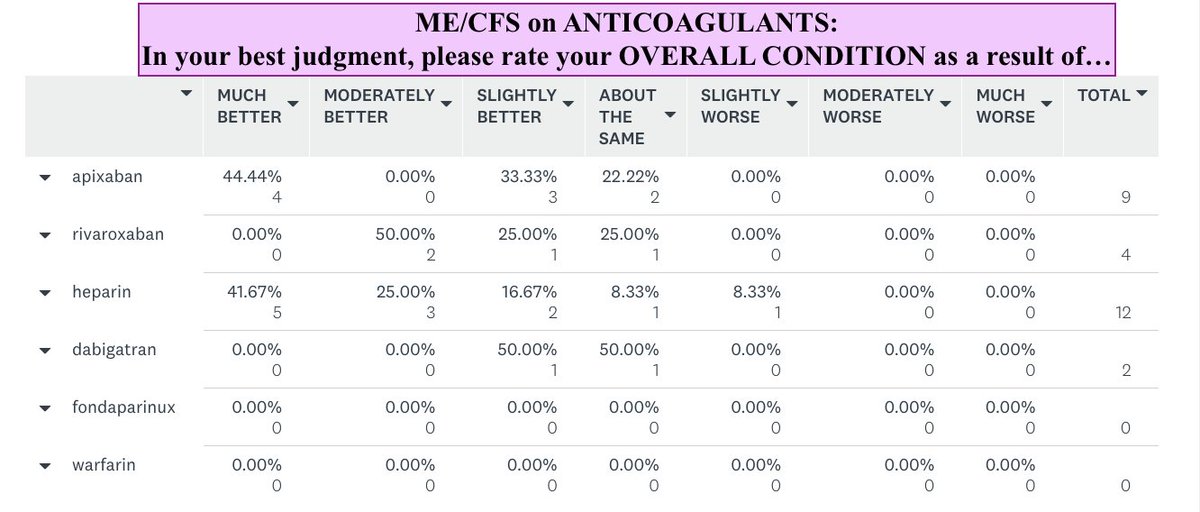
3) In #pwME, sample sizes were much smaller so I was unable to break down as many subgroups. I really need more #pwME to answer this survey. I know you're out there. 🥰 But it's interesting to note that HEPARIN was a shining star in both #pwME & #pwLC, helping almost 75%!
3) continued:
In #pwLC who took heparin + antiplatelets, 9 in 11 (82%) reported benefits & 87.5% reported "quite a few" of their symptoms significantly improved. Not sure why heparin might work better than oral anticoagulants. More studies with more participants needed obvs.
In #pwLC who took heparin + antiplatelets, 9 in 11 (82%) reported benefits & 87.5% reported "quite a few" of their symptoms significantly improved. Not sure why heparin might work better than oral anticoagulants. More studies with more participants needed obvs.
4) Quite a few w/ antiphospholipid syndrome are taking direct oral anticoagulants (DOACs). A large study came out last month concluding that those w/ APS should be on warfarin and not DOACs due to ⬆️ risk of clots in the latter. Talk w/ your dr about this.
jacc.org/doi/10.1016/j.…
jacc.org/doi/10.1016/j.…
5) NK & LK +/- SP stack up well here. No surprise considering that NK & LK directly degrade fibrin in clots whereas anticoagulants only prevent clot formation. ~65% improved on NK+SP (n=167) & LK (n=39). This doesn't even consider dose or formulation, so 65% is extra impressive.
6) Notably, 41% of lumbro respondents took Boluoke, the gold standard for LK, & none reported feeling worse. Respondents reported best results w/ Boluoke vs other LK brands. Almost 66% & 75% of #pwME & #pwLC who paired LK with SP or took LK + NK + SP improved.
There's lots more to go into, but I was excited & wanted to share a general overview of what I'm seeing so far in these treatments.😊If you know any #pwME or #pwLC on anticoagulants, antiplatelets, or NK/LK/SP, pls direct them to my #TREATME survey.
surveymonkey.com/r/TREATMEANDLC
surveymonkey.com/r/TREATMEANDLC
Disclaimer:
Remember this is all preliminary data & I'm not considering durations of treatment, doses or formulations here. I will do all that at a later date once I get more data.
Remember this is all preliminary data & I'm not considering durations of treatment, doses or formulations here. I will do all that at a later date once I get more data.
• • •
Missing some Tweet in this thread? You can try to
force a refresh