
1-Husband established w/a clinic in our town-
Same one that refused to treat my pain a few yrs ago after exacerbating my neck injury carrying firewood.
MD had told me I'd need a referral to a pain clinic as my pain was related to a chronic condition. 🤨
Husband given a brochure.
Same one that refused to treat my pain a few yrs ago after exacerbating my neck injury carrying firewood.
MD had told me I'd need a referral to a pain clinic as my pain was related to a chronic condition. 🤨
Husband given a brochure.



2-He then saw this in the exam room.
He took photos for me of all of this as he knows how they treated me in the past and he also knows about all the hypocrisy of what they say vs what they actually do when it comes to CPPs.
'PAIN TREATMENT ISN'T BLACK AND WHITE'
He took photos for me of all of this as he knows how they treated me in the past and he also knows about all the hypocrisy of what they say vs what they actually do when it comes to CPPs.
'PAIN TREATMENT ISN'T BLACK AND WHITE'

3-Following are close ups of the poster.

4-Exercise, listen to your body, do some internet searches, 'look within'...

5-Log your pain on an app. Your pain is likely just because you have poor posture and if that's not it you probably need therapy.
And obviously you've overlooked the power of natural, non medical options.
And obviously you've overlooked the power of natural, non medical options.
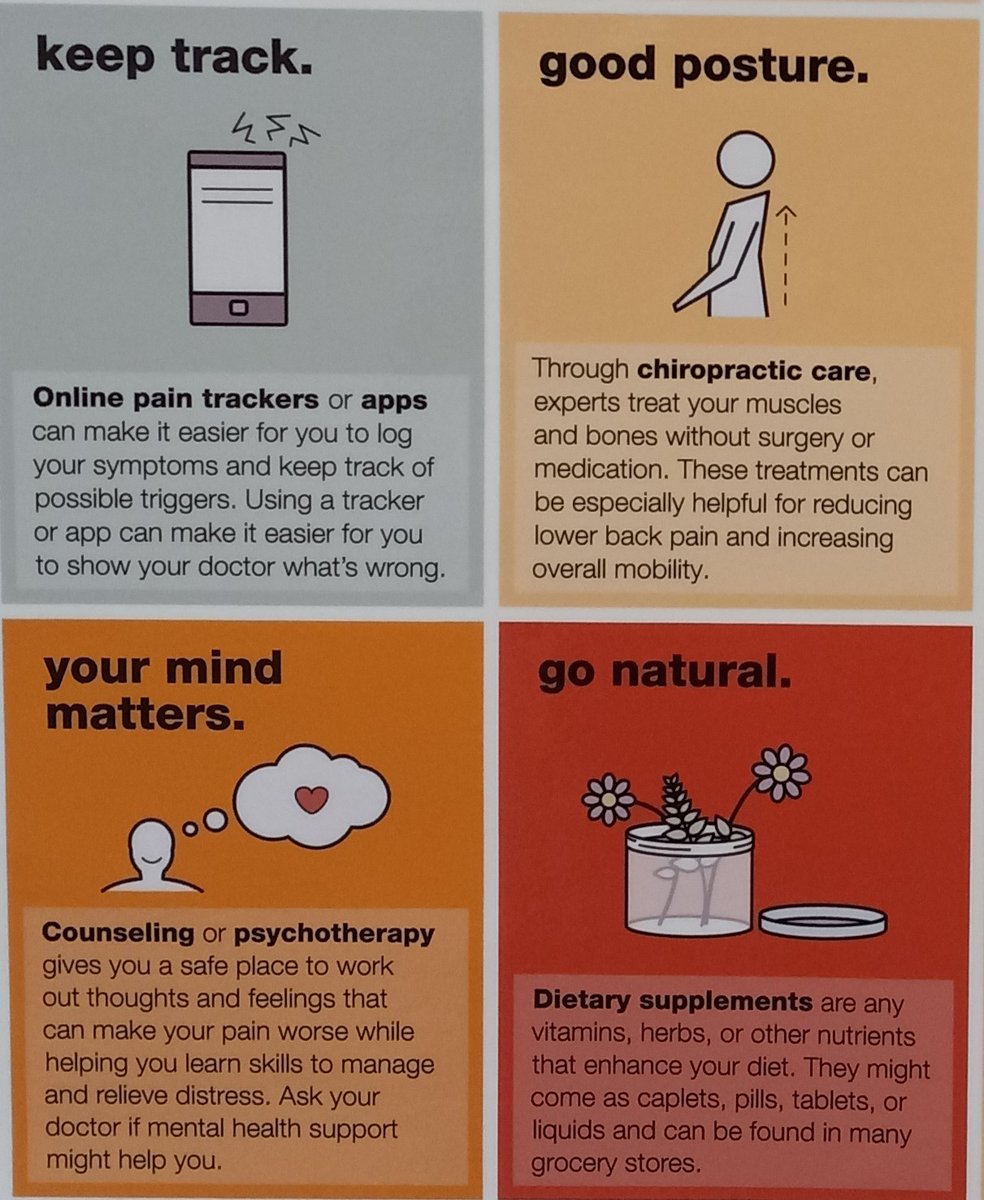
6-Stretch. You've probably just been laying around on the couch you malingering wretch.
You probably never even tried ice packs/heating pads or looked into getting yourself hooked up with a TCM doc.
Maybe you can just zap yourself out of it.
Why are you bothering us?
You probably never even tried ice packs/heating pads or looked into getting yourself hooked up with a TCM doc.
Maybe you can just zap yourself out of it.
Why are you bothering us?

7-I just want to point out that the Federally mandated brochure is a joke. #ChronicPain patients don't have any rights, especially the right to choose tx options. 🧐
Nor does their stupid poster mention discussing pain medicine options with a doctor at all. 🧐🤫
Nor does their stupid poster mention discussing pain medicine options with a doctor at all. 🧐🤫
• • •
Missing some Tweet in this thread? You can try to
force a refresh





