Reason # 76587 why lung #pocus is important: it can often give more information than CXR or CT Chest can. Case in point:
Elderly female on methotrexate and prednisone presenting with fever and cough.
Initial CXR:
Elderly female on methotrexate and prednisone presenting with fever and cough.
Initial CXR:
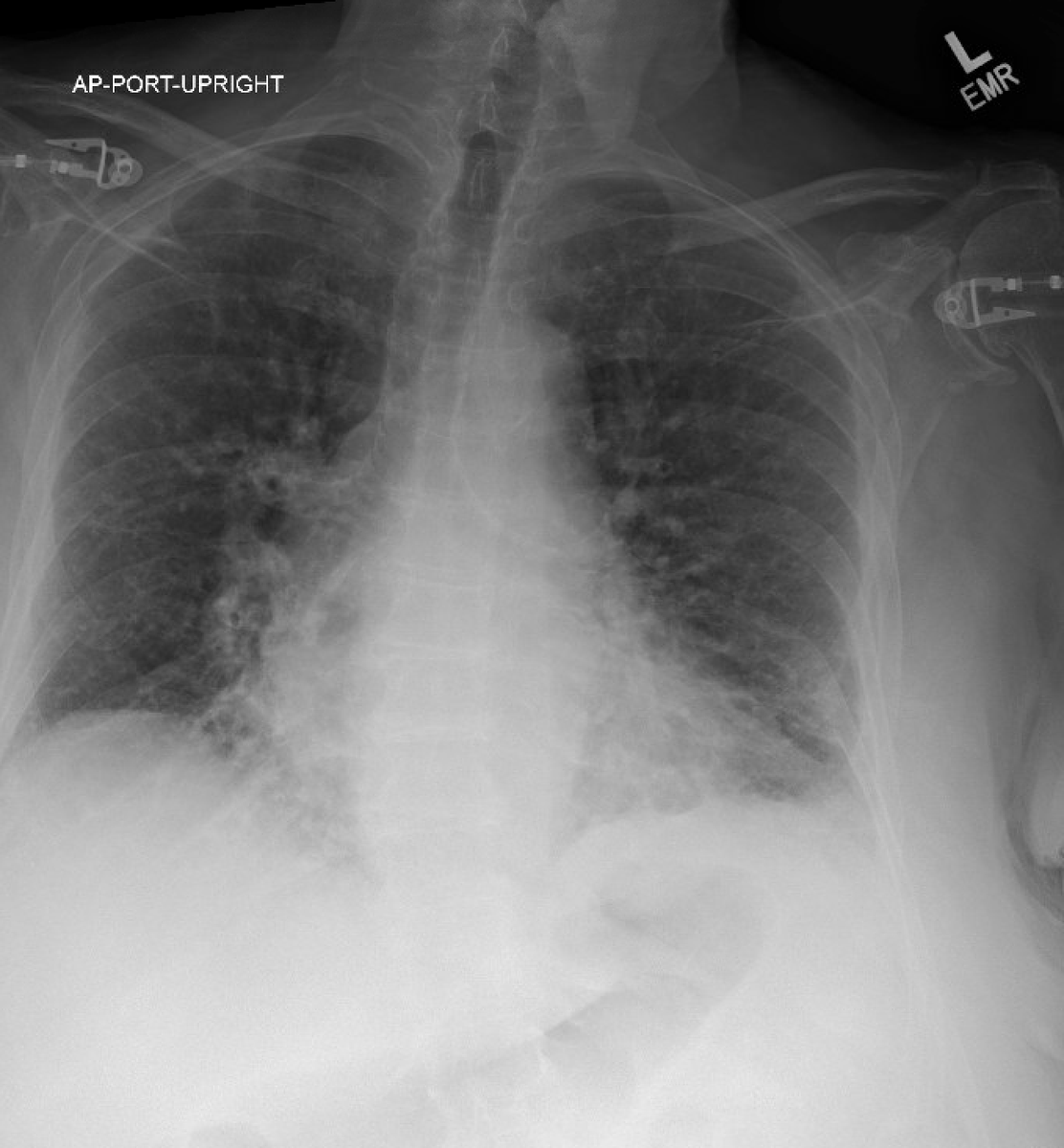
Read as "Bibasilar atelectasis." She was started on antibiotics. The following morning had abdominal pain and CT chest abdomen and pelvis ordered. CT chest seen here:
Grossly does not look too impressive. Radiologist read it as "no consolidations, scattered linear opacities." That afternoon seen by a physician skilled in lung #pocus. Left lung lateral lung seen here
Diffuse B lines with irregular pleura. Right lung seen here:
This patient has diffuse lung rockets with jagged irregular pleura and no consolidation. With lung #pocus the differential is narrowed significantly to:
- viral pneumonia
- ARDS
- pulmonary fibrosis
With her acute presentation, viral pneumonia is most likely.
- viral pneumonia
- ARDS
- pulmonary fibrosis
With her acute presentation, viral pneumonia is most likely.
A respiratory viral panel was ordered which confirmed Human metapneumovirus. Given her immunocompromised stated, this lung ultrasound could also be consistent with PJP pneumonia.
Human metapneumovirus - like many other respiratory viruses - can cause respiratory failure.
annalsofintensivecare.springeropen.com/articles/10.11…
annalsofintensivecare.springeropen.com/articles/10.11…
The key here is that a zoomed-in view of the pleura can clue you into the diagnosis that a CT may not. Diffuse lung rockets with jagged irregular pleura are most likely pulmonary fibrosis or viral pneumonia.
It is cases like these that make us wonder a lot about the sensitivity of pleural disease on CT scans, and if lung ultrasound is in fact the gold standard.
@LunaGargani @Wilkinsonjonny @iceman_ex @NephroP @POCUS_Society @PracticalPOCUS @POCUSpeek @IM_POCUS #FOAMed #MedEd
@LunaGargani @Wilkinsonjonny @iceman_ex @NephroP @POCUS_Society @PracticalPOCUS @POCUSpeek @IM_POCUS #FOAMed #MedEd
• • •
Missing some Tweet in this thread? You can try to
force a refresh