
One of the most important diagnostic tests in Cardiology to interpret is the EKG.
Here are my thoughts and notes. Will continue to this thread. Let me know what you think!
Thread #13: Inferior, Posterior, RV Infarction
#arjuncardiology #medtwitter #CardioTwitter #MedEd #IMG
Here are my thoughts and notes. Will continue to this thread. Let me know what you think!
Thread #13: Inferior, Posterior, RV Infarction
#arjuncardiology #medtwitter #CardioTwitter #MedEd #IMG
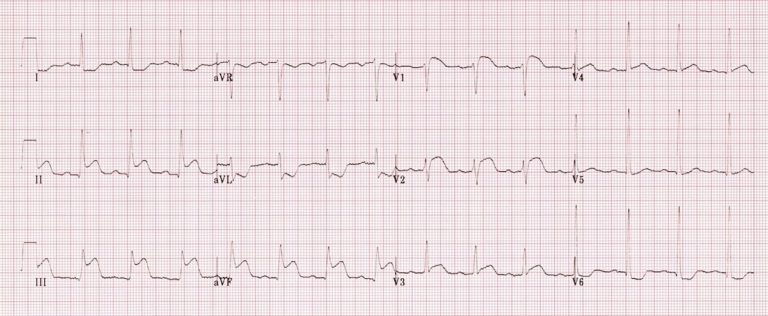
Inferior Wall Infarction:
- Diaphragmatic portion of the LV
- Will see changes in leads II, III, and aVF
- May produce abnormal Q-waves in these leads
- Generally caused by occlusion of the RCA; less commonly can occur with a left circumflex coronary obstruction
- Diaphragmatic portion of the LV
- Will see changes in leads II, III, and aVF
- May produce abnormal Q-waves in these leads
- Generally caused by occlusion of the RCA; less commonly can occur with a left circumflex coronary obstruction

Posterior Infarction:
- Occurs on the posterior (back) surface of the LV
- May be difficult to diagnose because characteristic abnormal ST elevations may no appear in any of the 12 conventional leads
- Tall R-waves and ST depressions can occur in V1 and V2
- Occurs on the posterior (back) surface of the LV
- May be difficult to diagnose because characteristic abnormal ST elevations may no appear in any of the 12 conventional leads
- Tall R-waves and ST depressions can occur in V1 and V2

Posterior Infarction:
- During evolving phase, deep T-wave inversions may appear in the posterior leads and anterior chest leads show reciprocally tall, positive T-waves
- During evolving phase, deep T-wave inversions may appear in the posterior leads and anterior chest leads show reciprocally tall, positive T-waves

Right Ventricular Infarction:
- Found in about 1/4 of cases of infero-posterior myocardial infarction
- Clinically, may have elevated central venous pressures (distended neck veins) because of abnormally high diastolic filling pressures in the right-side of the heart.
- Found in about 1/4 of cases of infero-posterior myocardial infarction
- Clinically, may have elevated central venous pressures (distended neck veins) because of abnormally high diastolic filling pressures in the right-side of the heart.
Right Ventricular Infarction:
- If damage to RV is severe, hypotension and cardiogenic shock can develop
- Can have AV conduction disturbances
- Many patients also have ST elevations in the leads reflecting the RV, such as V1 and V3R-V5R
- Need careful volume expansion
- If damage to RV is severe, hypotension and cardiogenic shock can develop
- Can have AV conduction disturbances
- Many patients also have ST elevations in the leads reflecting the RV, such as V1 and V3R-V5R
- Need careful volume expansion

Thanks to this amazing website for the graphics!
Stay tuned for the next thread!
litfl.com/inferior-stemi…
litfl.com/posterior-myoc…
litfl.com/right-ventricu…
Stay tuned for the next thread!
litfl.com/inferior-stemi…
litfl.com/posterior-myoc…
litfl.com/right-ventricu…
• • •
Missing some Tweet in this thread? You can try to
force a refresh














