Learning through mistakes.
(1/11) 38F. 90kg. No PMH. Fever x 3-4D ☞ body pains.
D6: frequent seizures. Multiple ASMs.
D7: CT head + CSF WNL.
D11: MR brain WNL (not shown).
D13: Repeat CSF WNL.
D16: Repeat MR Brain👇 faint b/l medial temporal hyperintensities.
Acyclovir ✅
(1/11) 38F. 90kg. No PMH. Fever x 3-4D ☞ body pains.
D6: frequent seizures. Multiple ASMs.
D7: CT head + CSF WNL.
D11: MR brain WNL (not shown).
D13: Repeat CSF WNL.
D16: Repeat MR Brain👇 faint b/l medial temporal hyperintensities.
Acyclovir ✅

(2/11) D19: shifted here.
Seizures ++, mostly over face w/ partial preserved consciousness.
Intubated. 4 ASMs ☞ Ketamine bolus ☞ infusion.
D19: IVIG + IV MPS also started.
Repeat CSF: routine normal. CSF BioFire -ve, including HSV. Acyclovir stopped.
Seizures ++, mostly over face w/ partial preserved consciousness.
Intubated. 4 ASMs ☞ Ketamine bolus ☞ infusion.
D19: IVIG + IV MPS also started.
Repeat CSF: routine normal. CSF BioFire -ve, including HSV. Acyclovir stopped.

(3/11) CSF autoimmune encephalitis panel -ve👇Serum paraneoplastic antibody panel -ve 👇


(4/11) Had aspirated.
BAL: BioFire: Acinetobacter+, Pseudomonas +, INFLUENZA A +👇
BAL: BioFire: Acinetobacter+, Pseudomonas +, INFLUENZA A +👇

(5/11) D24: repeat MR 👇 B/L medial temporal hyperintensities more prominent. Symmetrical.

(6/11):
Temporal lobe encephalitis can have varied etiologies.
academic.oup.com/cid/article/60…
Continuum: doi: 10.1212/CON.0000000000001244
Point to remember: Symmetrical medial temporal hyperintensities are mostly not herpetic.
Temporal lobe encephalitis can have varied etiologies.
academic.oup.com/cid/article/60…
Continuum: doi: 10.1212/CON.0000000000001244
Point to remember: Symmetrical medial temporal hyperintensities are mostly not herpetic.


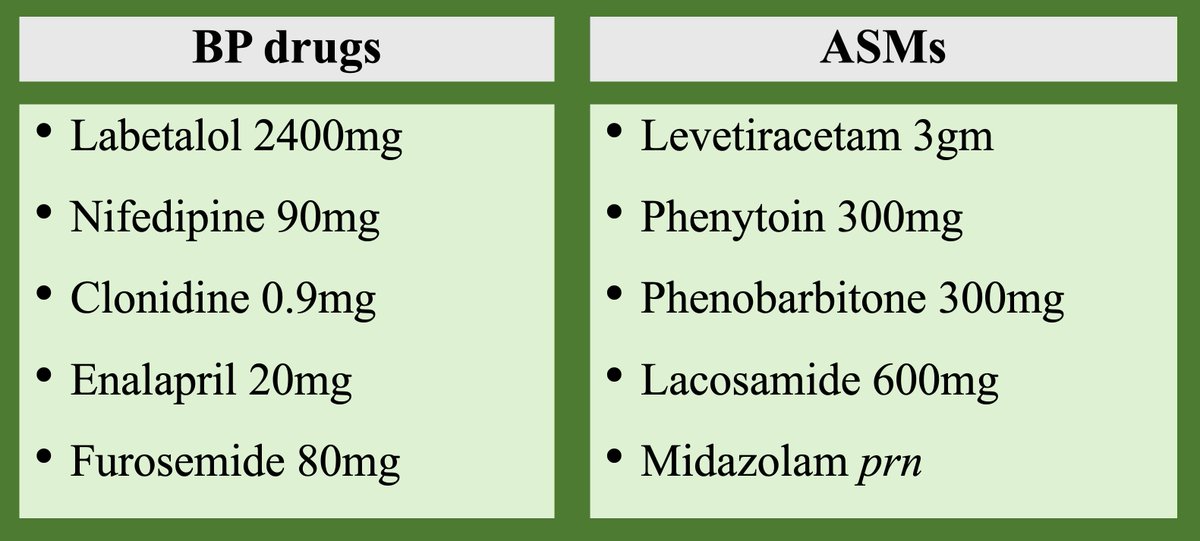
(7/11) Rx: On stopping Ketamine ☞ 48H Sz recurred. Again Ketamine x 48H + oral topiramate (TPM) loading (800mg x 24 hours) added to daily PHT 400mg, LEV 4gm, VPA 3gm, PHB 300mg.
Yes oral TPM can be used for loading in refractory SE.
onlinelibrary.wiley.com/doi/full/10.11…
Yes oral TPM can be used for loading in refractory SE.
onlinelibrary.wiley.com/doi/full/10.11…

(8/11) Topiramate w/ sodium valproate may have synergistic effects. frontiersin.org/articles/10.33…

9/11) But post TPM pt became dull/unarousable.
D32: urgent repeat MR👇, no additional findings.
D32: urgent repeat MR👇, no additional findings.

(10/11) Serum ammonia x 2, transaminases x 10 times.
We had made a MISTAKE. TPM can precipitate VPA induced encephalopathy.
onlinelibrary.wiley.com/doi/10.1111/j.…
We had made a MISTAKE. TPM can precipitate VPA induced encephalopathy.
onlinelibrary.wiley.com/doi/10.1111/j.…

(11/11) Stopped VPA + TPM. Nxt 24-48 hours alert. D40: discharged walking/smiling.
Our Dx: Febrile infection-related epilepsy syndrome (FIRES) triggered by Influenza A.
We would like expert comments & suggestions. Is the Dx correct?
#Medtwitter #Neurotwitter #FIRES #Radres
Our Dx: Febrile infection-related epilepsy syndrome (FIRES) triggered by Influenza A.
We would like expert comments & suggestions. Is the Dx correct?
#Medtwitter #Neurotwitter #FIRES #Radres
@LyellJ
@a_charidimou
@Jagan1234
@Narenmbbs
@hyderabaddoctor
@LD_McCullough
@theneurolander
@JayKinariwala
@Divyani_Garg
@DrTusharNeuro
@sudhir_kothari
@aksbnc
@piandro3142
@drpradeepck
@DrLKrishnamurt1
@jackie_palace
@Vishy89
@abgohel @MicieliA_MD
@ShadiYaghi2
@MicieliA_MD
@a_charidimou
@Jagan1234
@Narenmbbs
@hyderabaddoctor
@LD_McCullough
@theneurolander
@JayKinariwala
@Divyani_Garg
@DrTusharNeuro
@sudhir_kothari
@aksbnc
@piandro3142
@drpradeepck
@DrLKrishnamurt1
@jackie_palace
@Vishy89
@abgohel @MicieliA_MD
@ShadiYaghi2
@MicieliA_MD
@LyellJ @a_charidimou @Jagan1234 @Narenmbbs @hyderabaddoctor @LD_McCullough @theneurolander @JayKinariwala @Divyani_Garg @DrTusharNeuro @sudhir_kothari @aksbnc @piandro3142 @drpradeepck @DrLKrishnamurt1 @jackie_palace @Vishy89 @abgohel @MicieliA_MD @ShadiYaghi2 @teachplaygrub
@thecortexclub
@MohitAgNeurorad
@drSurjthVattoth
@EMiddlebrooksMD
@LorenzoPinelli
@theneuroradguy
@drbejoy2002
@drharunyildiz
@frankgaillard
@PeterGKranz
@samrad77
@daniel_gewolb
@sarbesh1984
@DrArpitaSahu
@BrentWeinberg
@drforamgala
@PhilipRChapman1
@thecortexclub
@MohitAgNeurorad
@drSurjthVattoth
@EMiddlebrooksMD
@LorenzoPinelli
@theneuroradguy
@drbejoy2002
@drharunyildiz
@frankgaillard
@PeterGKranz
@samrad77
@daniel_gewolb
@sarbesh1984
@DrArpitaSahu
@BrentWeinberg
@drforamgala
@PhilipRChapman1
@LyellJ @a_charidimou @Jagan1234 @Narenmbbs @hyderabaddoctor @LD_McCullough @theneurolander @JayKinariwala @Divyani_Garg @DrTusharNeuro @sudhir_kothari @aksbnc @piandro3142 @drpradeepck @DrLKrishnamurt1 @jackie_palace @Vishy89 @abgohel @MicieliA_MD @ShadiYaghi2 @teachplaygrub @thecortexclub @MohitAgNeurorad @drSurjthVattoth @EMiddlebrooksMD @LorenzoPinelli @theneuroradguy @drbejoy2002 @drharunyildiz @frankgaillard @ABStewardess
@drtimothyli
@BJegorovic
@PrathitKulkarni
@marignierro
@StaceyLClardy
@HuttoSpencer
@PavanBhargavaMD
@mdsebaslopez
@darshi_r
@CaseyJeffreysMD
@anneke_vdw
@monicamargoni
@EoinFlanagan14
@AaronBosterMD
@SaimaTCMD
@TheMOGProject
@drbarrysinger @rkchoi
@bobvarkey
@drtimothyli
@BJegorovic
@PrathitKulkarni
@marignierro
@StaceyLClardy
@HuttoSpencer
@PavanBhargavaMD
@mdsebaslopez
@darshi_r
@CaseyJeffreysMD
@anneke_vdw
@monicamargoni
@EoinFlanagan14
@AaronBosterMD
@SaimaTCMD
@TheMOGProject
@drbarrysinger @rkchoi
@bobvarkey
@LyellJ @a_charidimou @Jagan1234 @Narenmbbs @hyderabaddoctor @LD_McCullough @theneurolander @JayKinariwala @Divyani_Garg @DrTusharNeuro @sudhir_kothari @aksbnc @piandro3142 @drpradeepck @DrLKrishnamurt1 @jackie_palace @Vishy89 @abgohel @MicieliA_MD @ShadiYaghi2 @teachplaygrub @thecortexclub @MohitAgNeurorad @drSurjthVattoth @EMiddlebrooksMD @LorenzoPinelli @theneuroradguy @drbejoy2002 @drharunyildiz @frankgaillard @ABStewardess @drtimothyli @BJegorovic @PrathitKulkarni @marignierro @caseyalbin
@SunilAShethMD
@EricGoldsteinMD
@aartisarwal
@VMSilvera
@nihaal08
@drmankad
@cesaralvesneuro
@stikkman11
@draash
@JordiRoldanB @DrCindyCooper
@Sthanu5
@NicoGagelmann
@PulmCrit
@SunilAShethMD
@EricGoldsteinMD
@aartisarwal
@VMSilvera
@nihaal08
@drmankad
@cesaralvesneuro
@stikkman11
@draash
@JordiRoldanB @DrCindyCooper
@Sthanu5
@NicoGagelmann
@PulmCrit

• • •
Missing some Tweet in this thread? You can try to
force a refresh