
Regency Health | SGPGIMS | PMCH | BSMC | 𝕾𝖍𝖊𝖗𝖑𝖔𝖈𝖐𝖎𝖆𝖓 𝖎𝖓 𝖙𝖍𝖔𝖚𝖌𝖍𝖙𝖘 | 𝕎𝕒𝕥𝕤𝕠𝕟𝕚𝕒𝕟 𝕒𝕥 𝕓𝕖𝕕𝕤𝕚𝕕𝕖
 ❷
❷
 2️⃣History.
2️⃣History.
 38♀. 90kg.
38♀. 90kg. 
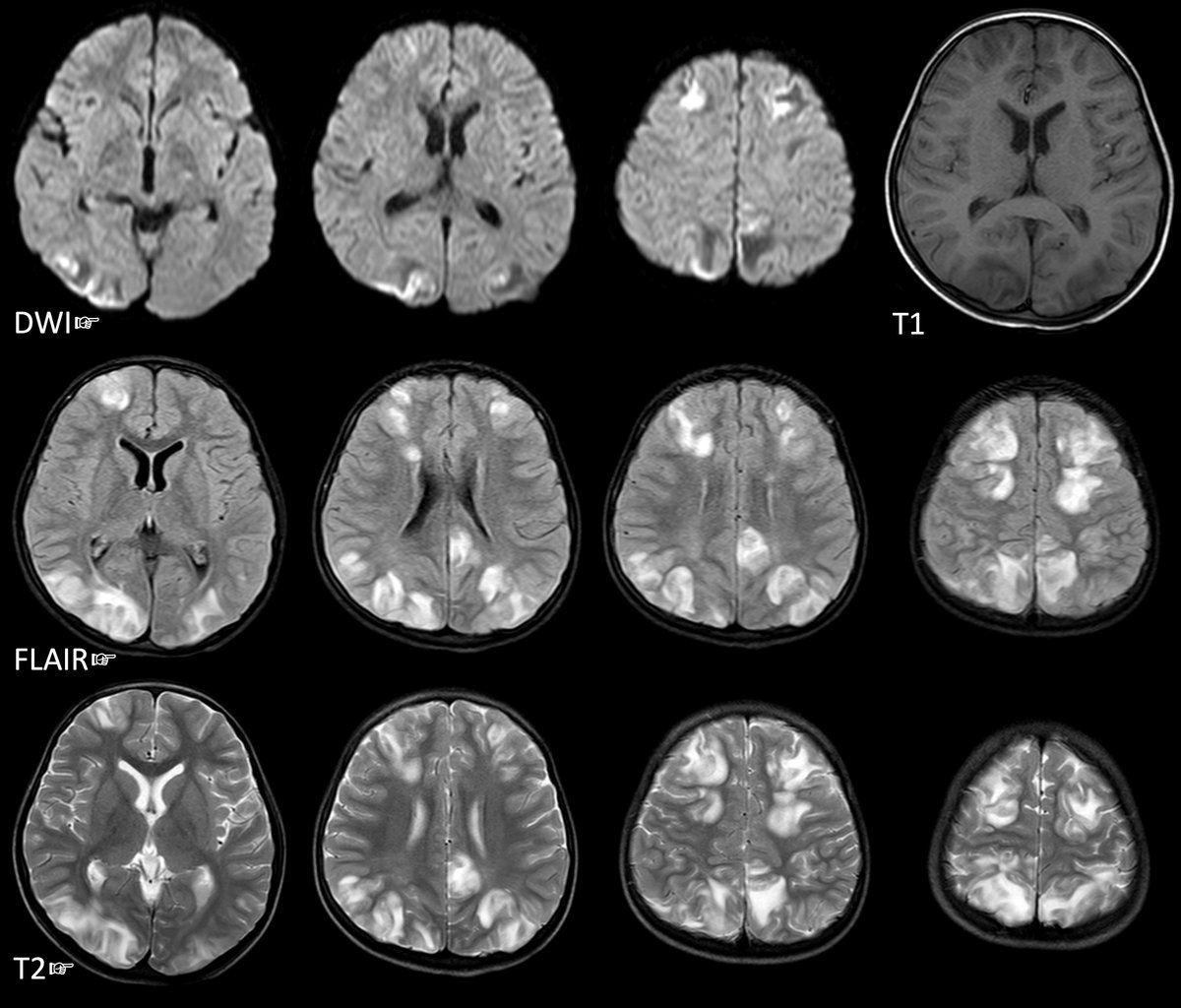
 These thoughts usually jump to the mind.
These thoughts usually jump to the mind. MR brain T2/T1 👇
MR brain T2/T1 👇
 She had come w/ some investigations done over past 6M.
She had come w/ some investigations done over past 6M.
 Taken to a nearby hospital. ↑ restless & agitation.
Taken to a nearby hospital. ↑ restless & agitation. 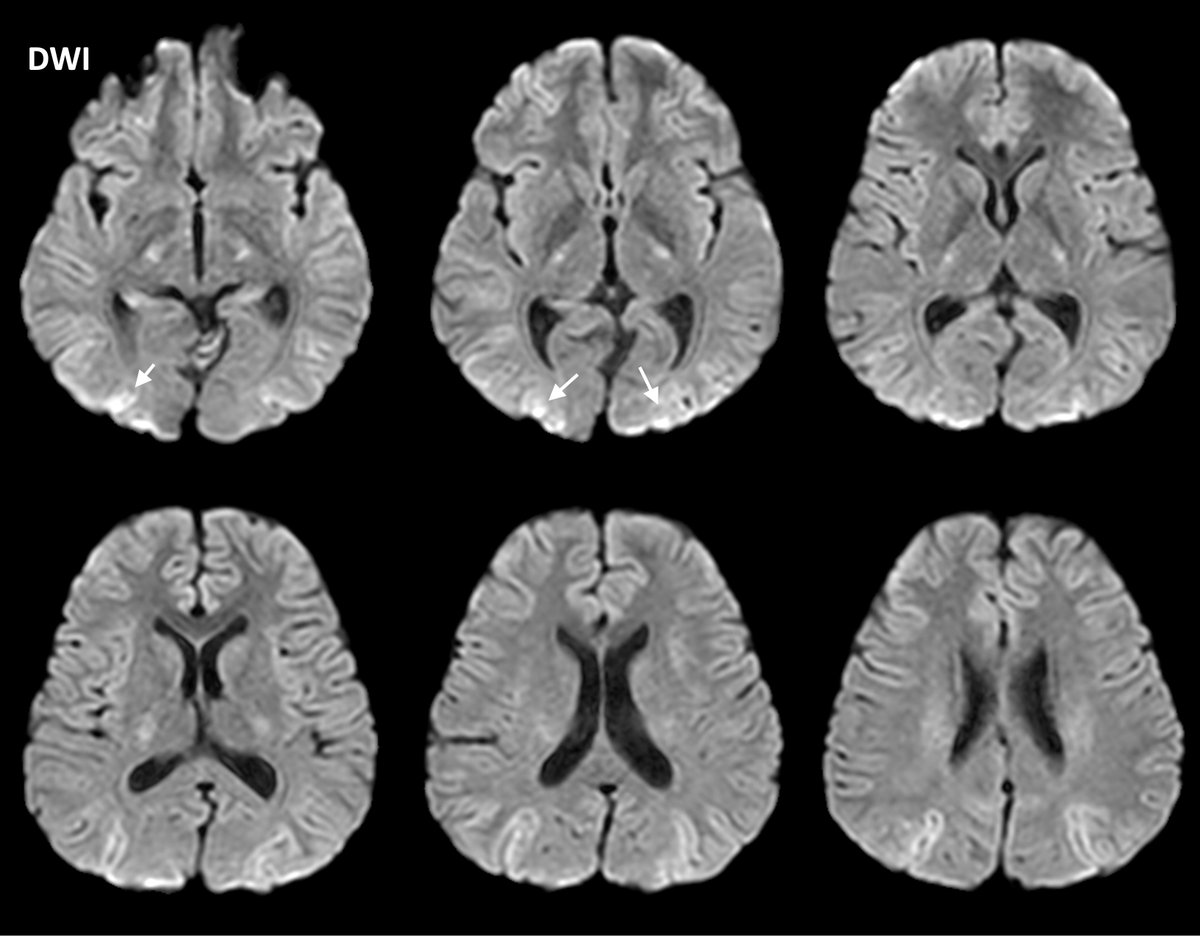
 Case 1: There was no Gad enhancement or restricted diffusion.
Case 1: There was no Gad enhancement or restricted diffusion. D2. Visited PHC.
D2. Visited PHC. 
 (2/11) D19: shifted here.
(2/11) D19: shifted here. 

 @thecortexclub @Brandon_Beaber @LyellJ @TylerAllisonMD @MohitAgNeurorad @marignierro @DrCindyCooper @a_charidimou @Jagan1234 @HuttoSpencer @VMSilvera @drSurjthVattoth @LorenzoPinelli @LyellJ @rkchoi @bobvarkey @caseyalbin @OligoclonalBand @StaceyLClardy @mdsebaslopez @Sthanu5
@thecortexclub @Brandon_Beaber @LyellJ @TylerAllisonMD @MohitAgNeurorad @marignierro @DrCindyCooper @a_charidimou @Jagan1234 @HuttoSpencer @VMSilvera @drSurjthVattoth @LorenzoPinelli @LyellJ @rkchoi @bobvarkey @caseyalbin @OligoclonalBand @StaceyLClardy @mdsebaslopez @Sthanu5
 8D later readmitted there w/ headache x 3D w/ mild rt ptosis. Again IVMPS x 3gm. Better. Again recurrence of headaches. Both times followup oral steroids not given. Came to us.
8D later readmitted there w/ headache x 3D w/ mild rt ptosis. Again IVMPS x 3gm. Better. Again recurrence of headaches. Both times followup oral steroids not given. Came to us.