Q for #medtwitter #cardiotwitter :
How many have noticed ECG being taken by nurses/students with this chest lead placement?
I see it so often but still gets on my nerves everytime!
Just curious if this is a common phenomenon?
How many have noticed ECG being taken by nurses/students with this chest lead placement?
I see it so often but still gets on my nerves everytime!
Just curious if this is a common phenomenon?

@anunay_cardio @AdiG1993 @abadkhan2002 @suheildhanse @Hragy @drjatinanand @DrGJustinPaul1 @DrRajeshG1 @ashwinrajenesh @djc795 @rallamee @just1doctorwala @meshaljoseph
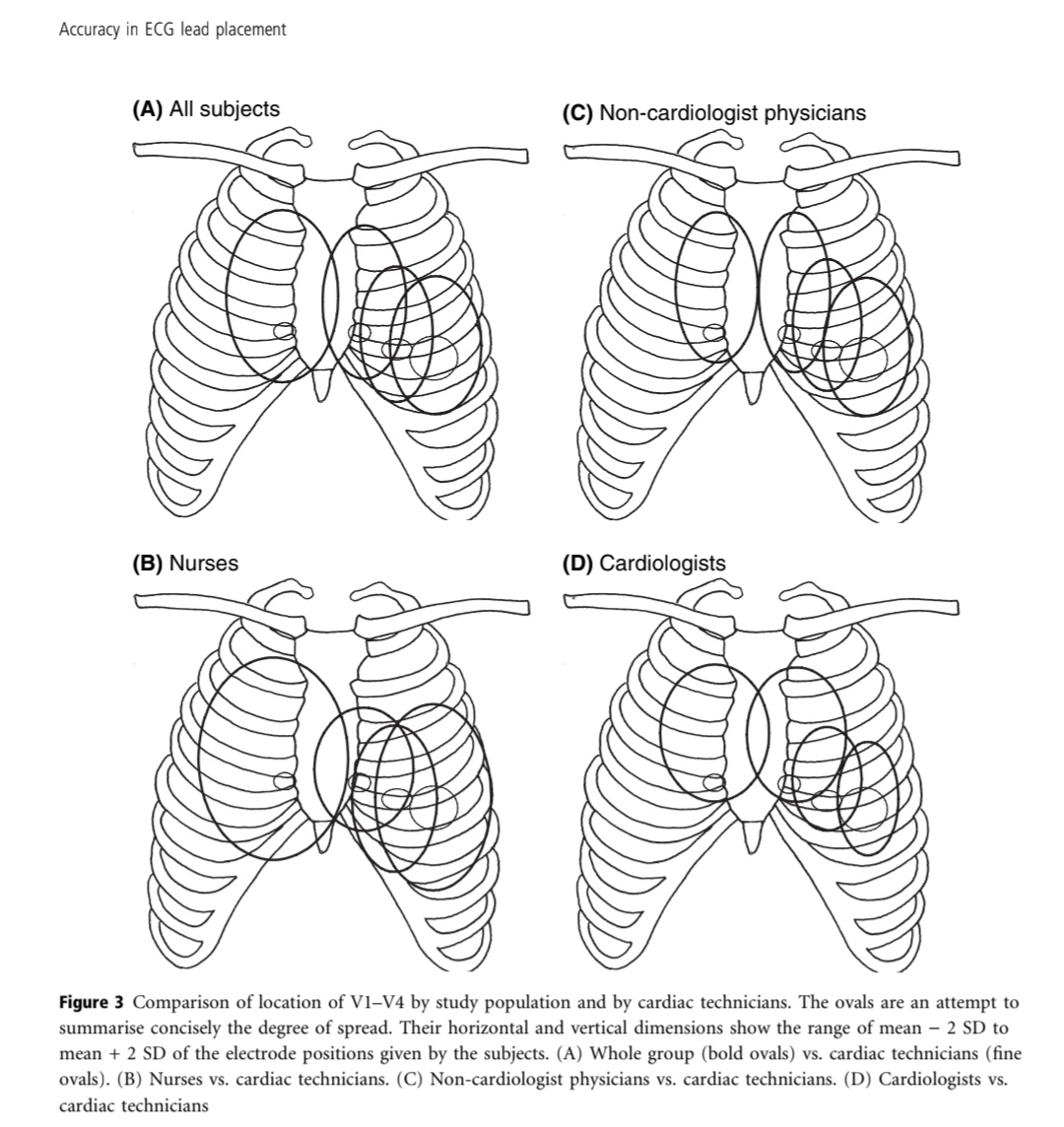
I am linking to am interesting article that shows that this lack of knowledge of accurate ECG lead placement extends even to cardiologists!
onlinelibrary.wiley.com/doi/abs/10.111…
DM if u want pdf..
onlinelibrary.wiley.com/doi/abs/10.111…
DM if u want pdf..

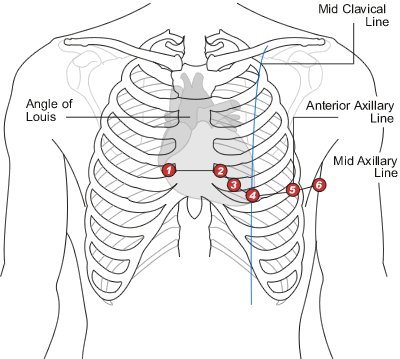
For those who are asking for the correct lead positioning this is the figure to remember 👇
This is a fantastic workaround for when suction cups refuse to stay in position, either due the shape of the chest, mammary tissue, etc.
Thanks to @ashwinrajenesh for this!
Thanks to @ashwinrajenesh for this!
https://twitter.com/ashwinrajenesh/status/1647994586684592130?t=Hd8mJaWihnqm2uho_4025A&s=19
• • •
Missing some Tweet in this thread? You can try to
force a refresh