
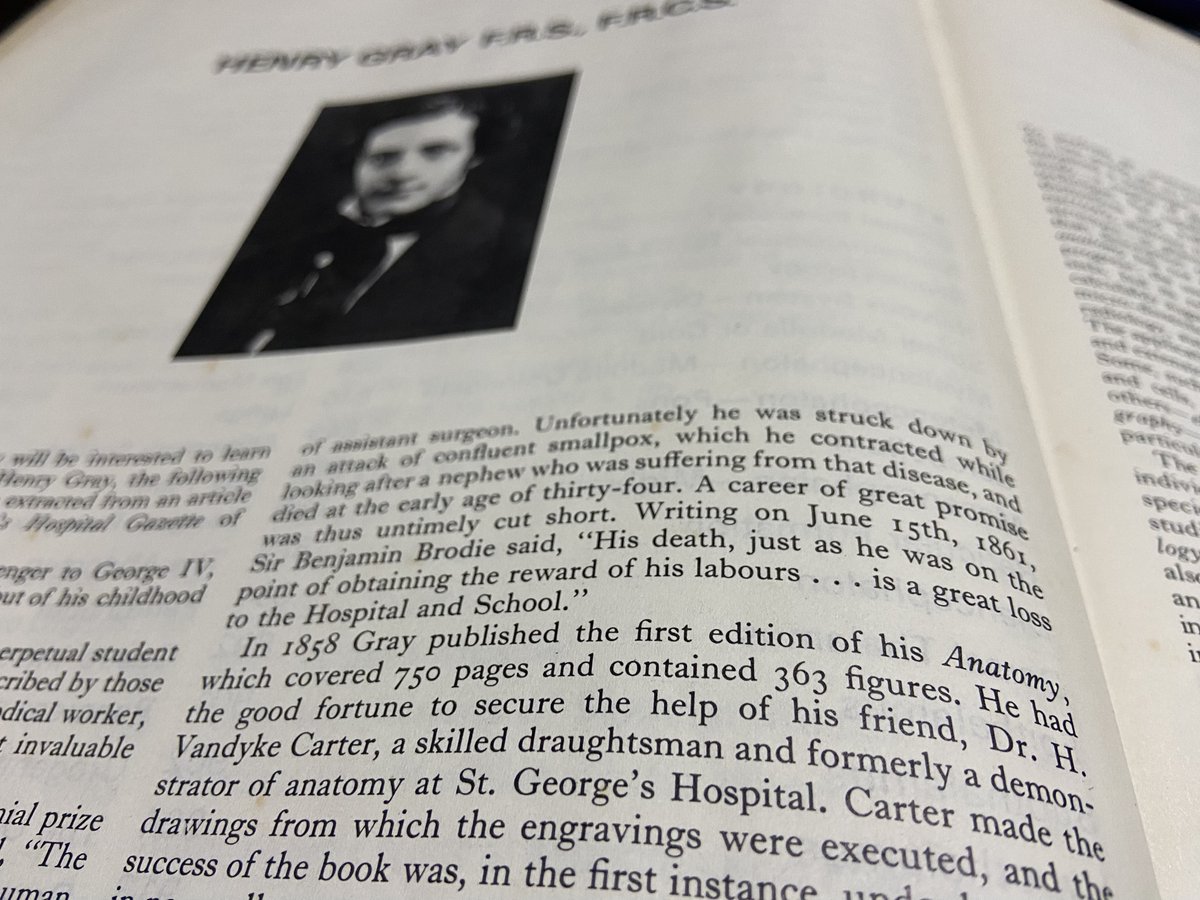
This century old portrait is from the library of my Grant Medical College in Mumbai!
Who is he? How is he related to the famous Gray's Anatomy? How did he end up here?
A fascinating story from the archives of medicine!
Who is he? How is he related to the famous Gray's Anatomy? How did he end up here?
A fascinating story from the archives of medicine!

The gentleman in this fine portrait is Henry Vandyke Carter. If you have ever seen earlier editions of Gray's anatomy, you will have noticed the gorgeous illustrations in them. Arguably, these illustrations made Gray's Anatomy a superlative text
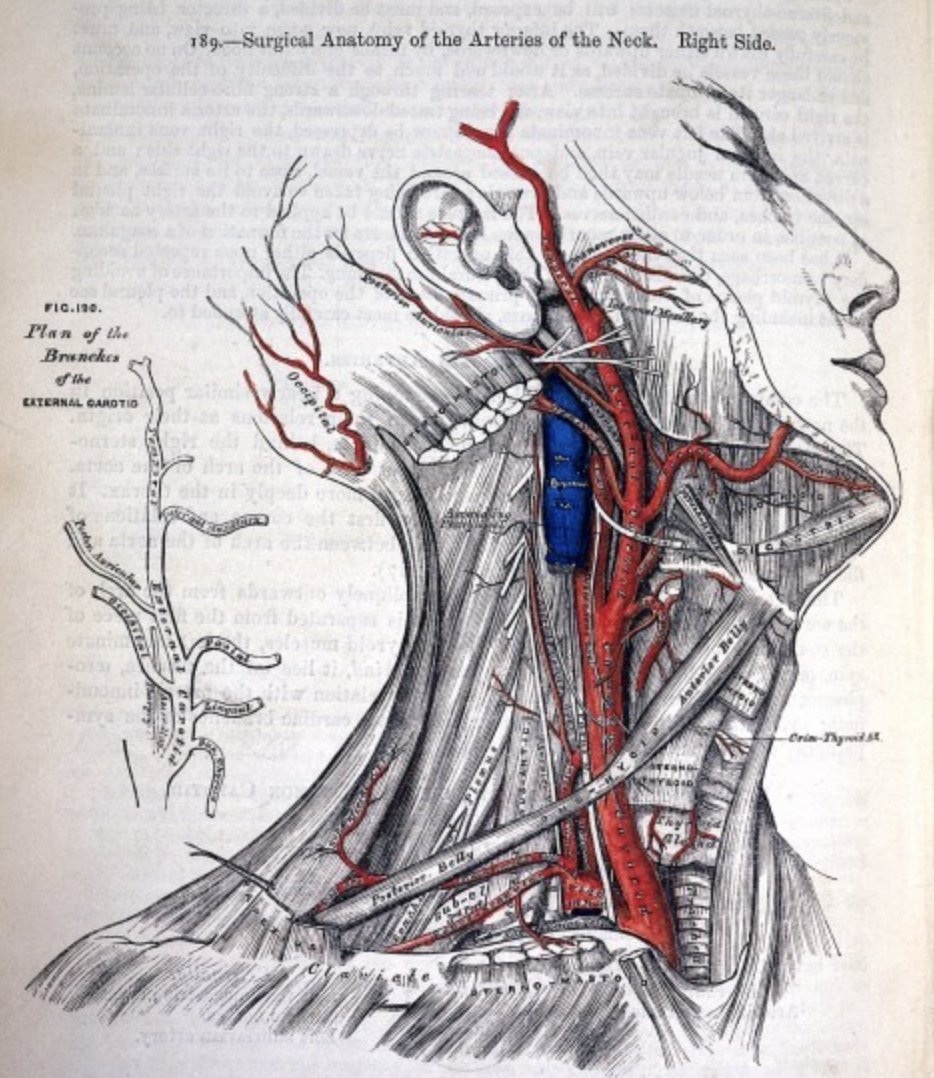
The artist to those illustrations is Van Dyke Carter!
Instead of following convention of labelling structures outside the diagram, see how he labels them on the diagram itself, making out so easy to understand!
Instead of following convention of labelling structures outside the diagram, see how he labels them on the diagram itself, making out so easy to understand!

Also, he apparently directly engraved these, in a reverse mirror image, so they could be printed directly! Genius!
Also, he decided the fictional dissected subjects with compassion rather than the grotesque open eyed and open mouthed images prevalent back in the day!
Also, he decided the fictional dissected subjects with compassion rather than the grotesque open eyed and open mouthed images prevalent back in the day!
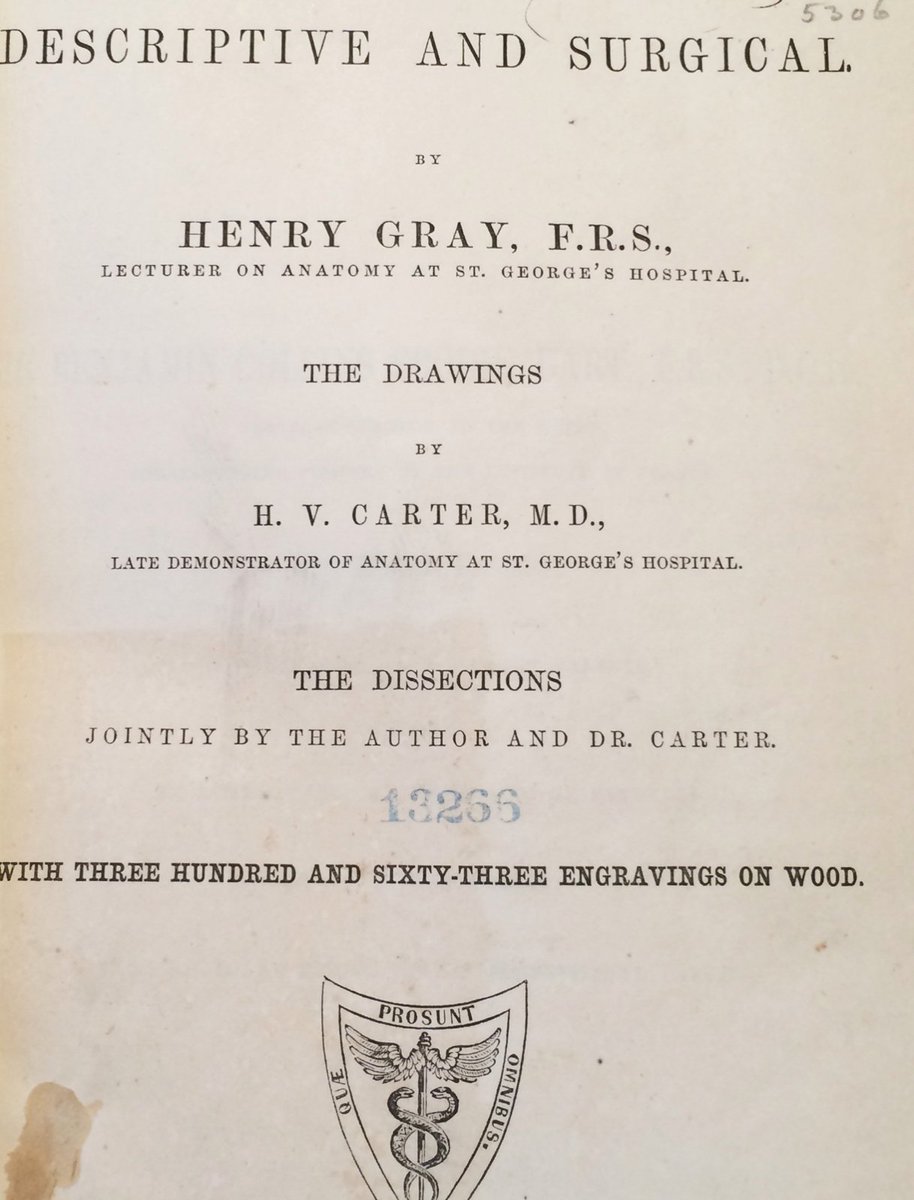
However, it seems that as the book became famous, Henry Gray, flamboyant as he was, took all the credit and limelight, leaving the reticent genius Carter in the shadows.
See the name of Gray, Bold and larger font
See the name of Gray, Bold and larger font
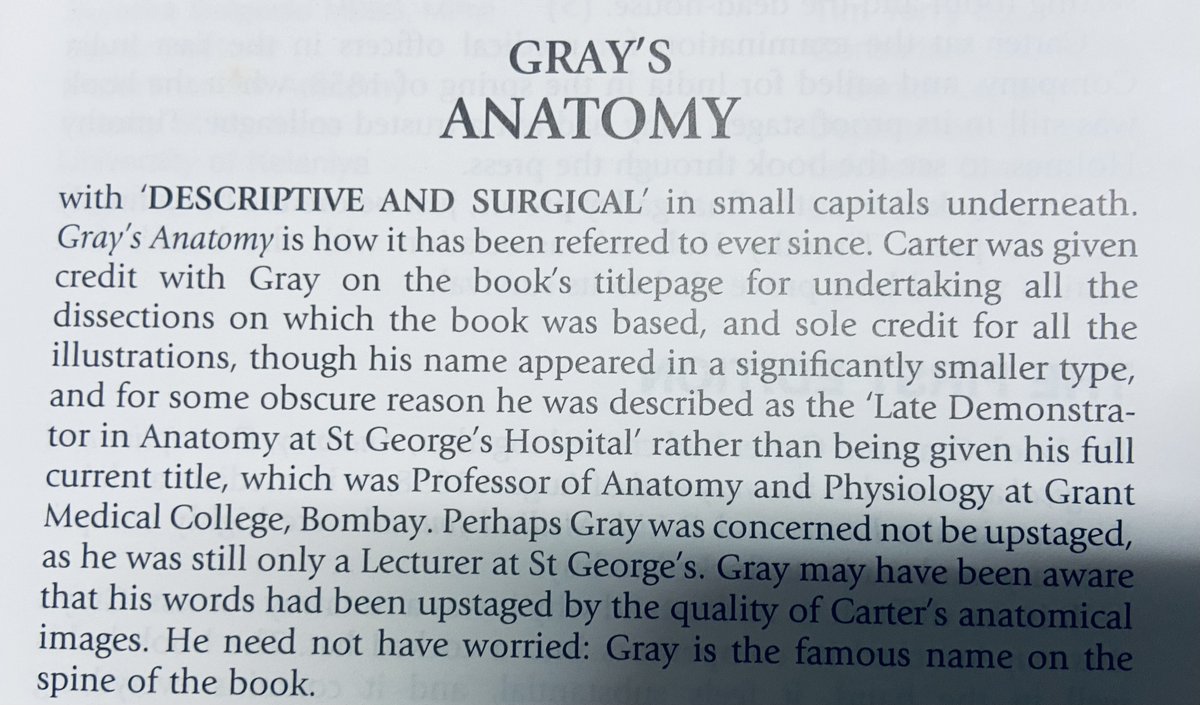
This part of the story is even covered in the edition of Gray's that I (didn't) read! The 40th edition!
The other image is from Papa's edition of the book, which also takes cognisance of Carter's genius, even if hidden between lines
The other image is from Papa's edition of the book, which also takes cognisance of Carter's genius, even if hidden between lines
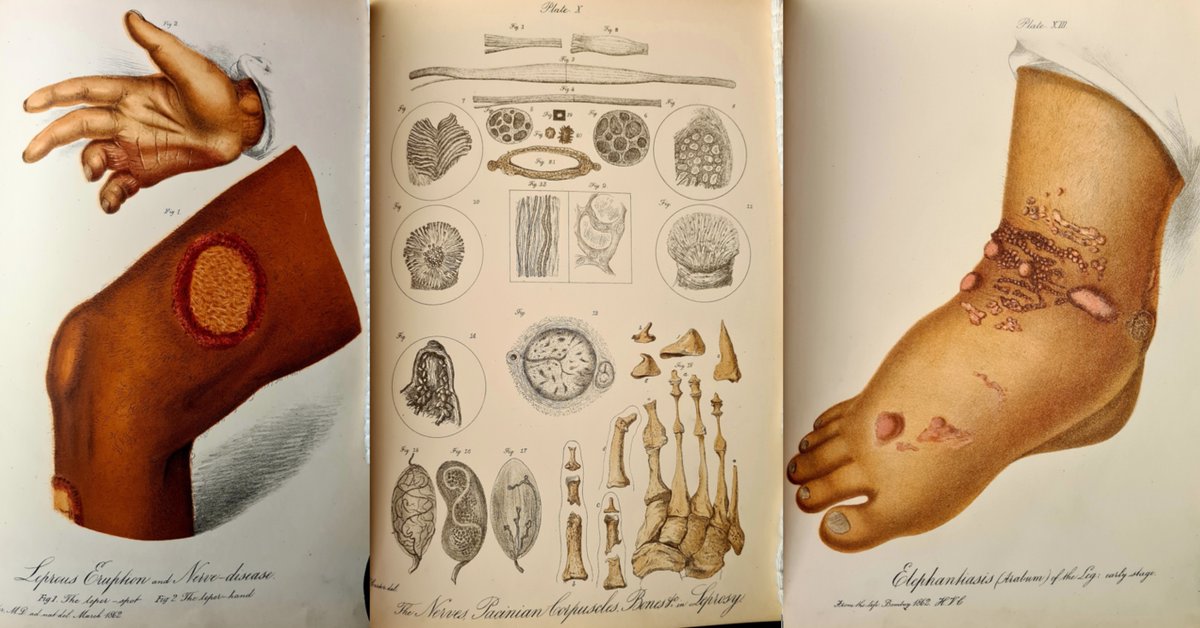
Frustrated, Carter came to Mumbai (the Bombay) to my institution! Grant Medical College! Here he served as the dean, and did some great work in an eclectic collections of fields
Seminal work on Mycetoma, Relapsing Fever, Leprosy, Kidney Stones!
List of deans of GMC, Mumbai. See number 7!

Coming back to our portrait! It's a beautiful portrait with Van Dyke Carter posing stoically. One may believe that with all the achievements, he moved on from Gray's Anatomy
But if you take a closer look at his bookshelf
You see this! Gray and Carter, in equal prestige on the spine of the book!
You see this! Gray and Carter, in equal prestige on the spine of the book!

This along with a number of portraits will soon find their way into museum built on our campus!
There are so many more fascinating stories I have stumbled across from my century and a half year old Grant Medical College!
#MedTwitter #Mumbai
There are so many more fascinating stories I have stumbled across from my century and a half year old Grant Medical College!
#MedTwitter #Mumbai
• • •
Missing some Tweet in this thread? You can try to
force a refresh








