Top Ten slides from day 1 of the @BSHeartFailure meeting @JubileeHospital conference centre in Glasgow. A 🧵for all in the #HF MDT
1) Hypotension with HF meds- less than you might think- mean SBP⬇️ at 6m 1-2mmHg with eplerenone & 2mmHg with SGLT2i
Slide shown by @_antocannata
1) Hypotension with HF meds- less than you might think- mean SBP⬇️ at 6m 1-2mmHg with eplerenone & 2mmHg with SGLT2i
Slide shown by @_antocannata

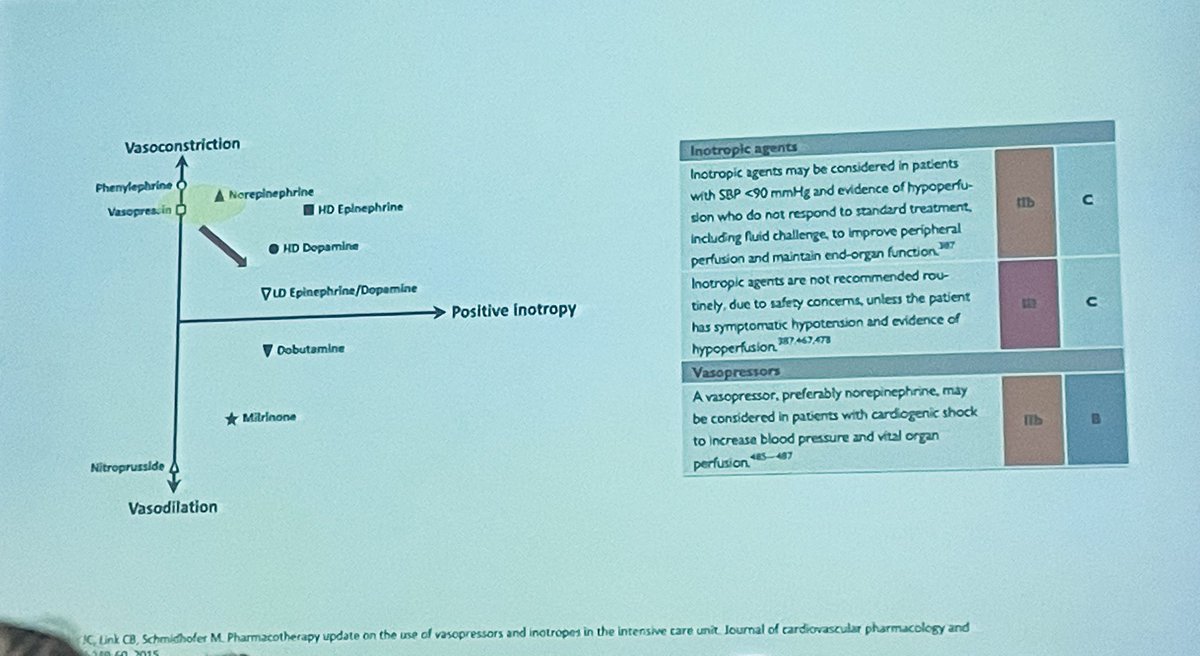
2) Summary slide of drugs that may be used in shock plotted on a scale of inotropy and vasoconstriction.
Slide shown as part of a case discussion by Daniel Doherty #HF
Slide shown as part of a case discussion by Daniel Doherty #HF
3) A reminder that the absence of crackles and a normal CXR do not exclude ⬆️ PCWP
Slide shown by @drpmcampbell #HF
Slide shown by @drpmcampbell #HF

4) Summary of sensitivity and specificity of various signs and symptoms for congestion
Slide shown by Ross Campbell #HF
Slide shown by Ross Campbell #HF

5) Reminder of the gains to be made by OMT in #HF - 5 yrs of life gained vs no therapy
Slide shown by @TheresaMcDonag3
Slide shown by @TheresaMcDonag3

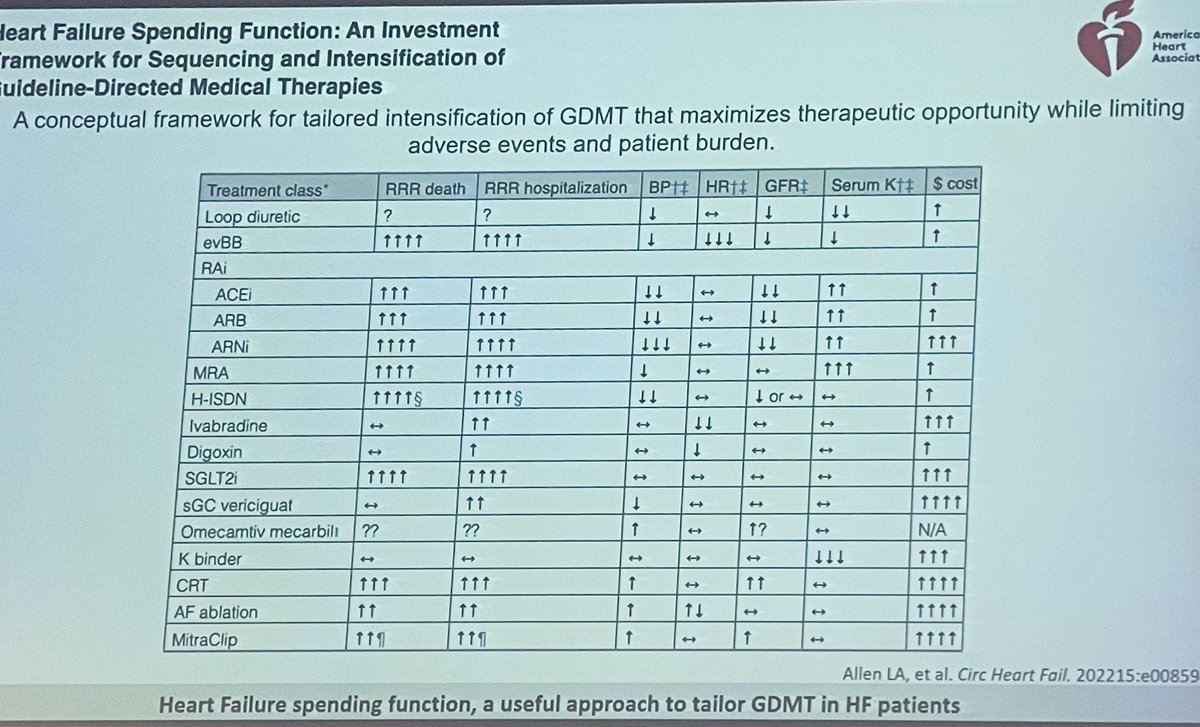
6) Comprehensive summary table of effects of different #HF drugs on HR/BP/egfr/K
Slide shown by @_antocannata
Slide shown by @_antocannata
7) How sensitive & specific is ferritin as a surrogate for iron deficiency?
Slide shown by @JJCuthbert
Slide shown by @JJCuthbert

8) Has the #HF world taken a wrong turn? Should we be more focused on TSAT?
Slide shown by @JJCuthbert
Slide shown by @JJCuthbert

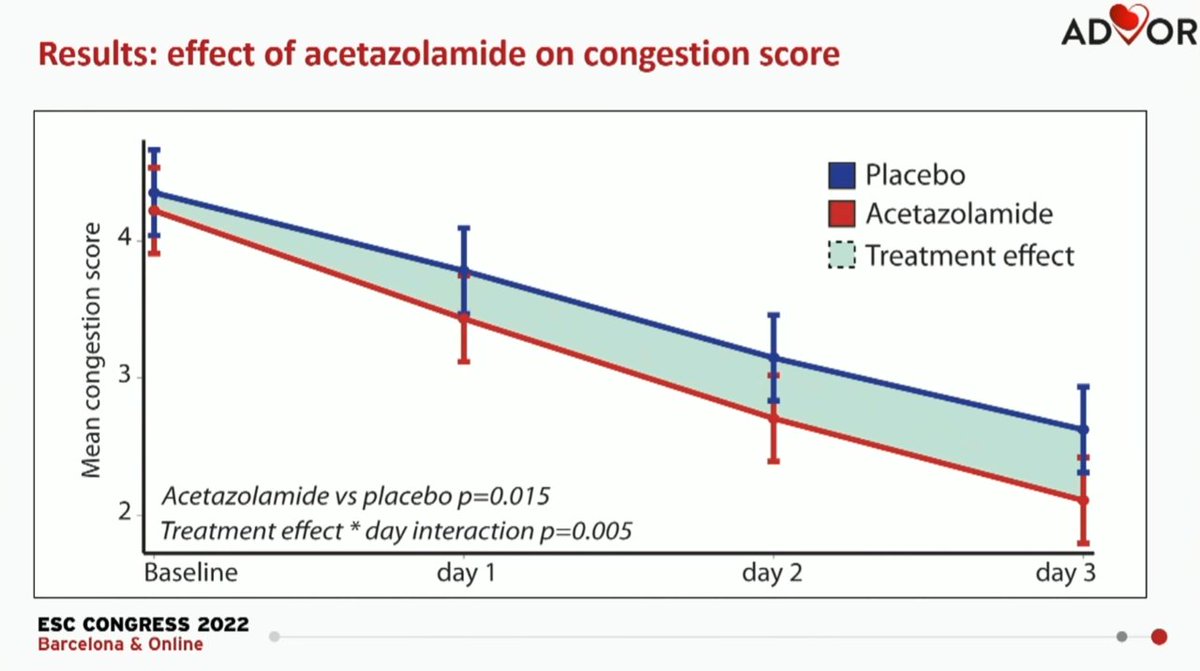
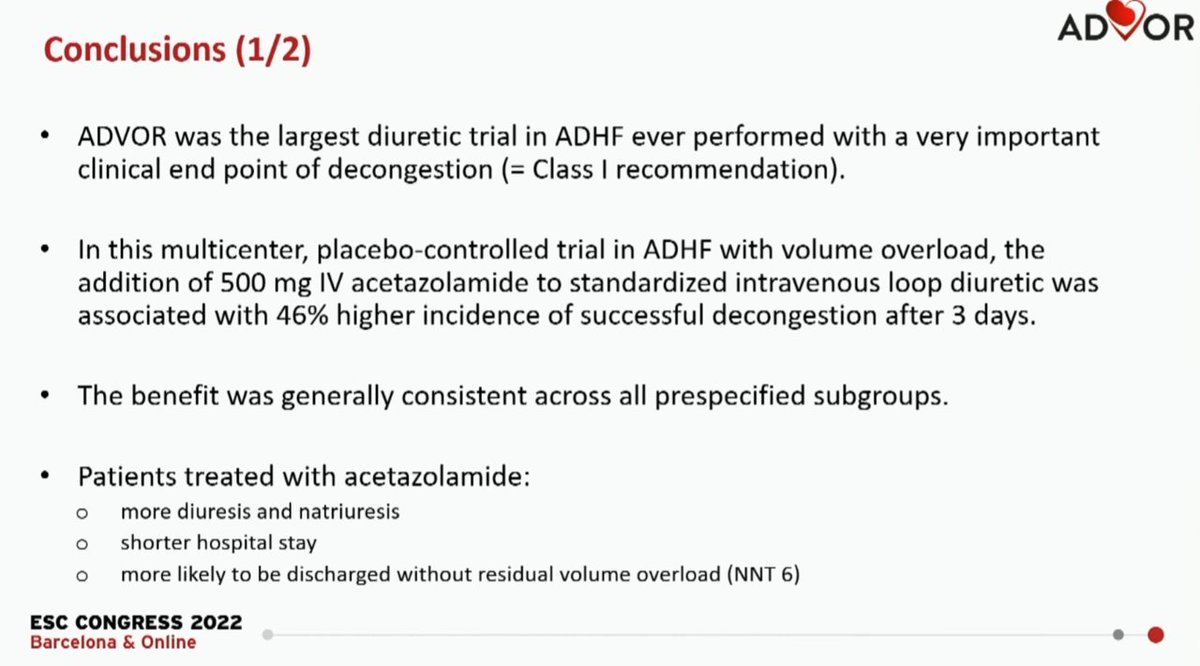
9) Strengths and weaknesses of ADVOR
Shown by Ross Campbell
Shown by Ross Campbell

10) Could CRT be useful for HFpEF? Still theoretical at present but interesting concept
Slide shown by Zaheer Yousef
Slide shown by Zaheer Yousef

Finally an honorary mention to @markcpetrie20 and @ProfDConnelly for a fabulous interactive case discussion & including a tribute to May 4th
https://twitter.com/profdconnelly/status/1654183082457542657
• • •
Missing some Tweet in this thread? You can try to
force a refresh