Navigating the binary gender paradigm - experiences of trans 🏳️⚧️ and gender expansive physicians at #SAEM23
⭐️Is there a problem?
⭐️What do we do?
From our work ➡️ jamanetwork.com/journals/jaman… @JarmanAF
🧵
⭐️Is there a problem?
⭐️What do we do?
From our work ➡️ jamanetwork.com/journals/jaman… @JarmanAF
🧵
We *know* trans/gender expansive patients don’t have same access or experience in healthcare. We *know* there’s stigma in healthcare delivery pubmed.ncbi.nlm.nih.gov/24184160/
It turns out that physicians also experience stigma and transphobia in the workplace jamanetwork.com/journals/jaman… (2/)
It turns out that physicians also experience stigma and transphobia in the workplace jamanetwork.com/journals/jaman… (2/)
In fact, teaching in MEDICAL SCHOOLS / TRAINING conflates being trans/gender expansive with being mentally ill - not good for patients, also harmful for T/GE clinicians. Leads to burnout and ⬇️representation in medicine (3/) 


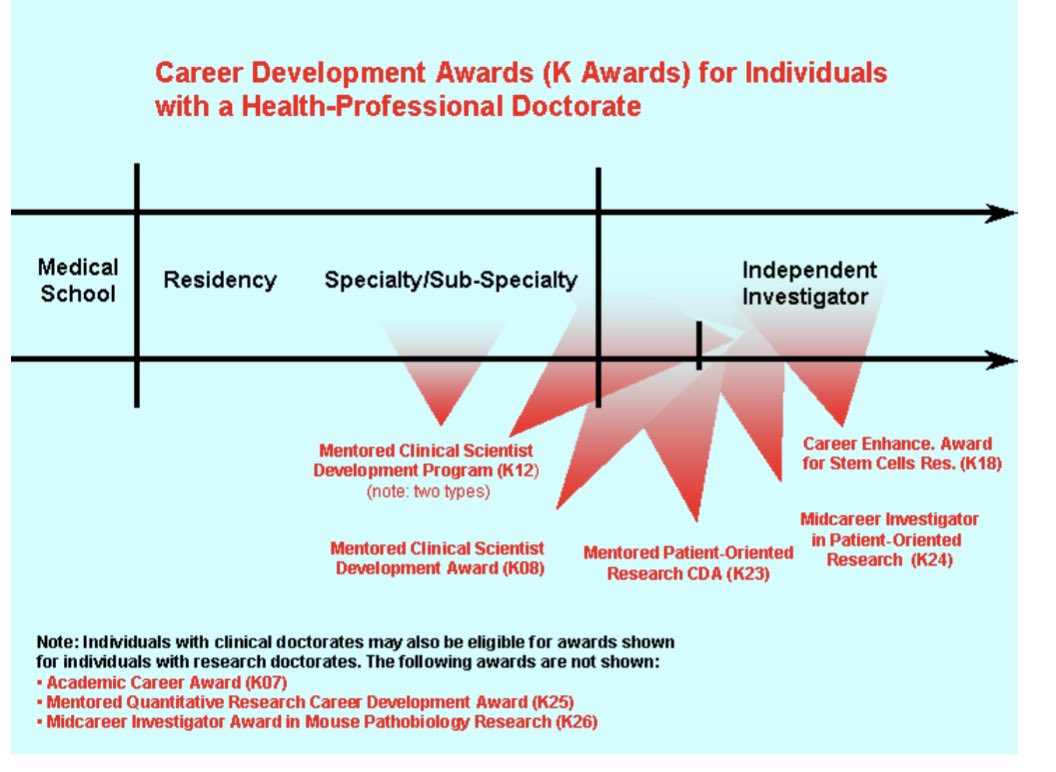
It often starts with oversimplification of sex, which is then dichotomized. But it’s more complicated.
Gender is often confused with sex, almost always dichotomized (neglecting gender expansive folk), & punished if gender expression doesn’t fit binary model (4/)
Gender is often confused with sex, almost always dichotomized (neglecting gender expansive folk), & punished if gender expression doesn’t fit binary model (4/)




In our study, we found there were several things people/programs/institutions could do to mitigate the stigma & negative experience.
1. Anticipate you will train and work with trans&gender expansive people. (And it’s totally likely/possible you won’t know they’re T/GE) (/5)
1. Anticipate you will train and work with trans&gender expansive people. (And it’s totally likely/possible you won’t know they’re T/GE) (/5)



It only takes a quick look on EM physician social media forums to see blatant transphobia. I’m our study, people discussed the harmful effects of witnessing this in clinical settings. JUST. BE. NICE. (And not transphobic) (/6)

But also think about the challenges incoming trainees and colleagues may face
⭐️being outed
⭐️name changes
⭐️physical spaces (/7)
⭐️being outed
⭐️name changes
⭐️physical spaces (/7)



Normalize giving pronouns and show signs of support.
LGBTQ+ people often look for these things as a signal of safety. It will also cause way fewer headaches and harm later. (/8)
LGBTQ+ people often look for these things as a signal of safety. It will also cause way fewer headaches and harm later. (/8)


For example, outing new residents/fellows on match day was an important theme in our study (& once this happened, people have trouble NOT misgendering them).
⭐️ask pronouns, name, and if you can use their eras picture before you tweet it out /hang it in the hospital (/9)
⭐️ask pronouns, name, and if you can use their eras picture before you tweet it out /hang it in the hospital (/9)


Understand that transitioning is particularly complicated during medical training with diplomas and licenses, EHRs. Work with your institution to build a toolkit medscape.com/viewarticle/94… (/9)
Tell all the trainees and employees where accessible gender, neutral, bathrooms, and locker rooms (so people don’t have to out themselves by asking AND so they can guide patients) (/10)
Think about the power you hold (even Med students hold power). When you correct misgendering, show that your space is a safe space it MATTERS (/11)


• • •
Missing some Tweet in this thread? You can try to
force a refresh