Are you considering going down the investigator route 🤓 in EM? Then you probably want to know about K awards. Some highlights from our panel at #SAEM23 🧵
What are early career K awards?
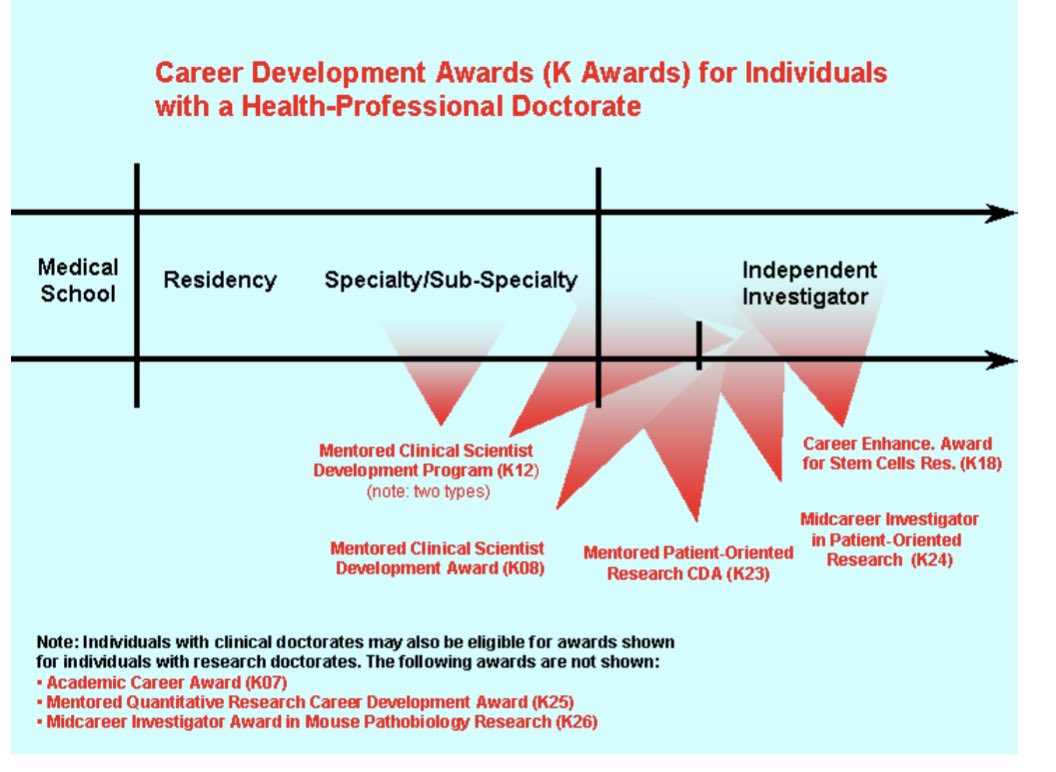
⭐️ career development awards
⭐️focus on developing research skills to turn you into an independent investigator
✌️broad types: institutional (k12/kl2) and individual awards (eg k08,k23)
researchtraining.nih.gov/programs/caree… (2/x)
⭐️ career development awards
⭐️focus on developing research skills to turn you into an independent investigator
✌️broad types: institutional (k12/kl2) and individual awards (eg k08,k23)
researchtraining.nih.gov/programs/caree… (2/x)
💵K awards fund you (mostly) to have time to do research, learn, and apply for grants.
⭐️commit to 75% research/25% clinical
➡️”funds” 75% research time (capped at 75-125k depending on institution)-ie institution on hook for salary cap gap
⬇️ 💵 for project (~25-40k/year) (4/)
⭐️commit to 75% research/25% clinical
➡️”funds” 75% research time (capped at 75-125k depending on institution)-ie institution on hook for salary cap gap
⬇️ 💵 for project (~25-40k/year) (4/)
Is a K award right for you?
⭐️answer is individual , some people may be ready to go straight to an R01 or similar award
⭐️needs to fill gap in knowledge/skills to advance in research
⭐️goal to become independently funded researcher (5/)
⭐️answer is individual , some people may be ready to go straight to an R01 or similar award
⭐️needs to fill gap in knowledge/skills to advance in research
⭐️goal to become independently funded researcher (5/)
How do you get a K award?
Lots of different paths, some of our common themes were
⭐️mentorship
⭐️institution
⭐️prelim pubs/data
⭐️protected time
⭐️children/family
⭐️rejection
⭐️reluctance
⭐️fellowships/training
⭐️”atypical” paths
⭐️finding your niche (6/)
Lots of different paths, some of our common themes were
⭐️mentorship
⭐️institution
⭐️prelim pubs/data
⭐️protected time
⭐️children/family
⭐️rejection
⭐️reluctance
⭐️fellowships/training
⭐️”atypical” paths
⭐️finding your niche (6/)
Mentorship is key
✅ For K awards,a “mentor” must be someone with individual NIH funding
✅They don’t get salary support for their mentoring so need to believe in mentorship and growing academic researchers
✅should have a shared specialization in trainee area of research
(7/)
✅ For K awards,a “mentor” must be someone with individual NIH funding
✅They don’t get salary support for their mentoring so need to believe in mentorship and growing academic researchers
✅should have a shared specialization in trainee area of research
(7/)


Institutional support
⭐️b/c a Ks cost dept (salary cap gap) they must be on board and “write” a powerful letter of support
⭐️find a place that values growing EM research. peers can make you better (eg @emschoenfeld prompted me to apply for K12 & hooked me up w/great mentor (8/)
⭐️b/c a Ks cost dept (salary cap gap) they must be on board and “write” a powerful letter of support
⭐️find a place that values growing EM research. peers can make you better (eg @emschoenfeld prompted me to apply for K12 & hooked me up w/great mentor (8/)

Protected (“academic”) time is important. It’s how you get and maintain grants and get research done. It’s helpful if you have some BEFORE you get a K to get the K (a research fellowship or some sweet deal) (/9)
Preliminary data and collaboration is important. Shows your project is feasible and that your team will give you adequate support. Building networks and collaborations can never start too early (/10)

⭐️Rejection. Embrace it. It will happen and it can make you better. Use the feedback
⭐️look at lots of funded Ks. The more you read, the more you will see the patters of success (hint: it’s a game) (/11)
⭐️look at lots of funded Ks. The more you read, the more you will see the patters of success (hint: it’s a game) (/11)
There are TONS of websites with rich resources and FAQs about Ks. About timelines (example) ctsi.wakehealth.edu/service/k-awar… (/12)
• • •
Missing some Tweet in this thread? You can try to
force a refresh