
We tested live Omicron BA.2.86 subvariant isolated from a South African swab. As you'll see below, it was lurking somewhere for over a year, then started to spread rather slowly, maybe because it evolved similar immune escape to what is circulating now, but no better.
Here are representative results of sera from vaccinated people with breakthrough Omicron infection (subvariants BA.1, BA.4/5, and XBB family) from what we found: 

We didn't find large differences in how these viruses replicated either. Similar size of infection foci after 20 hours (top) and cytopathic effect after 72 hours of infection (bottom) relative to XBB.1.5.

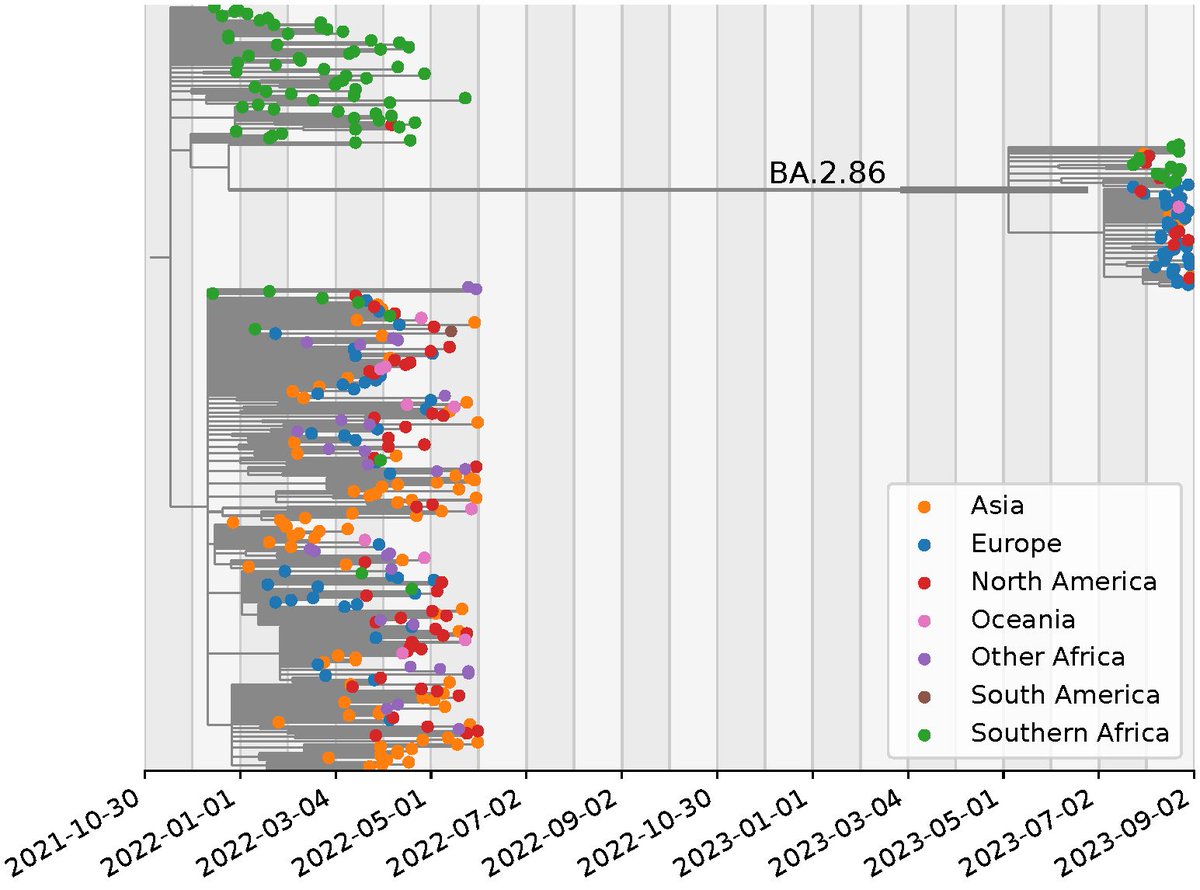
@richardneher did an analysis of where this variant may have come from
As you can see, BA.2.86 most closely resembles the sequences circulating in Southern Africa in early 2022. It then evolves but does not spread for over a year.
As you can see, BA.2.86 most closely resembles the sequences circulating in Southern Africa in early 2022. It then evolves but does not spread for over a year.
Based on these results, this variant is not a game changer. Our neut results are roughly similar to @BarouchLab, @BenjMurrell, and @yunlong_cao, though we saw less differences than @yunlong_cao and didn't see something that would indicate different infectivity vs. XBB.1.5
The long time this subvariant spent gaining mutations without spreading is likely because it was either a long infection in someone immunosuppressed or in an animal reservoir. We've seen these kinds of infections before:
medrxiv.org/content/10.110…
medrxiv.org/content/10.110…
I would like to thank @KhadijaKhan24, @richardneher, the folks at the South African NICD, @Tuliodna and the great team who made this study happen.
• • •
Missing some Tweet in this thread? You can try to
force a refresh






