1/Do you feel there’s a back-log of findings in a spine MRI report?
Everyone talks about discs & facets, but not everyone talks about the endplates
Do you?
Do you need to talk about degenerative changes (Modic changes) of the endplates?
Here’s thread w/all you need to know!
Everyone talks about discs & facets, but not everyone talks about the endplates
Do you?
Do you need to talk about degenerative changes (Modic changes) of the endplates?
Here’s thread w/all you need to know!

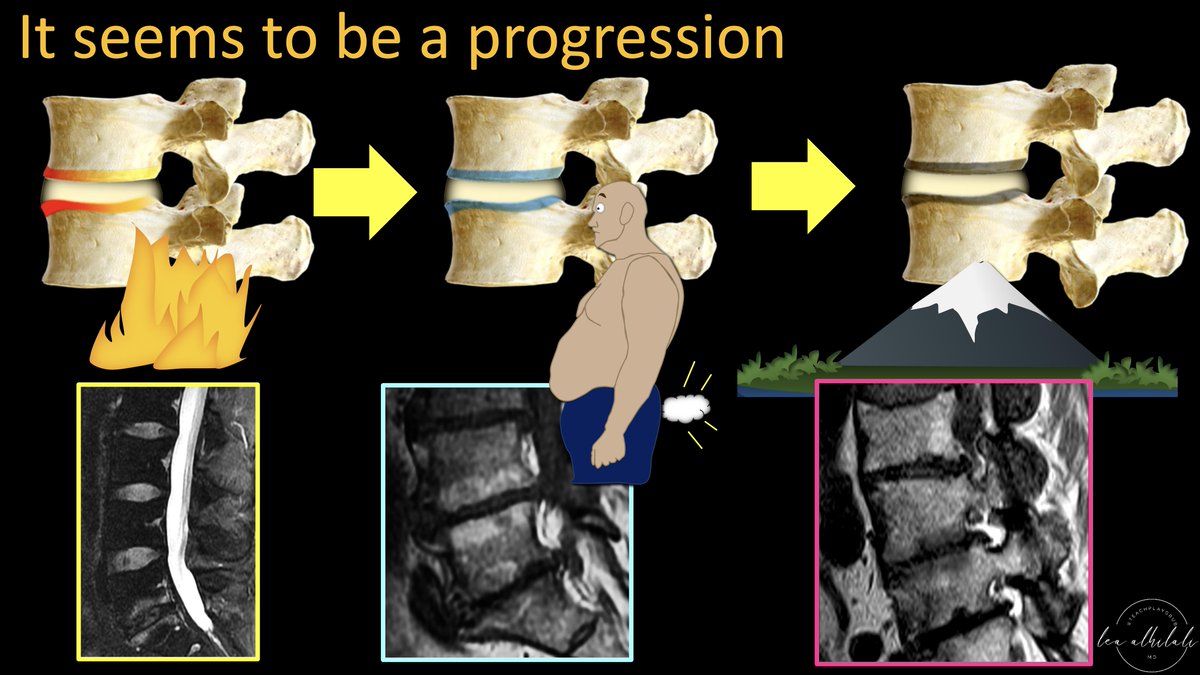
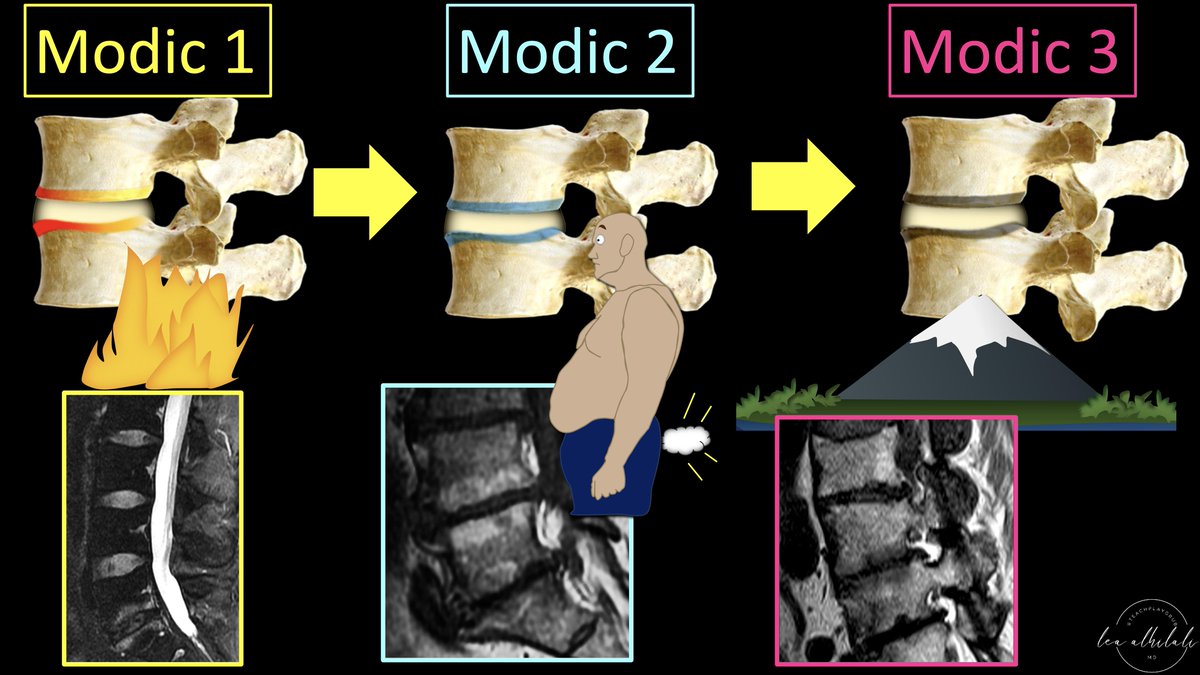
2/Over 30 years ago, Modic et al. found there were 3 types of degenerative endplate changes:
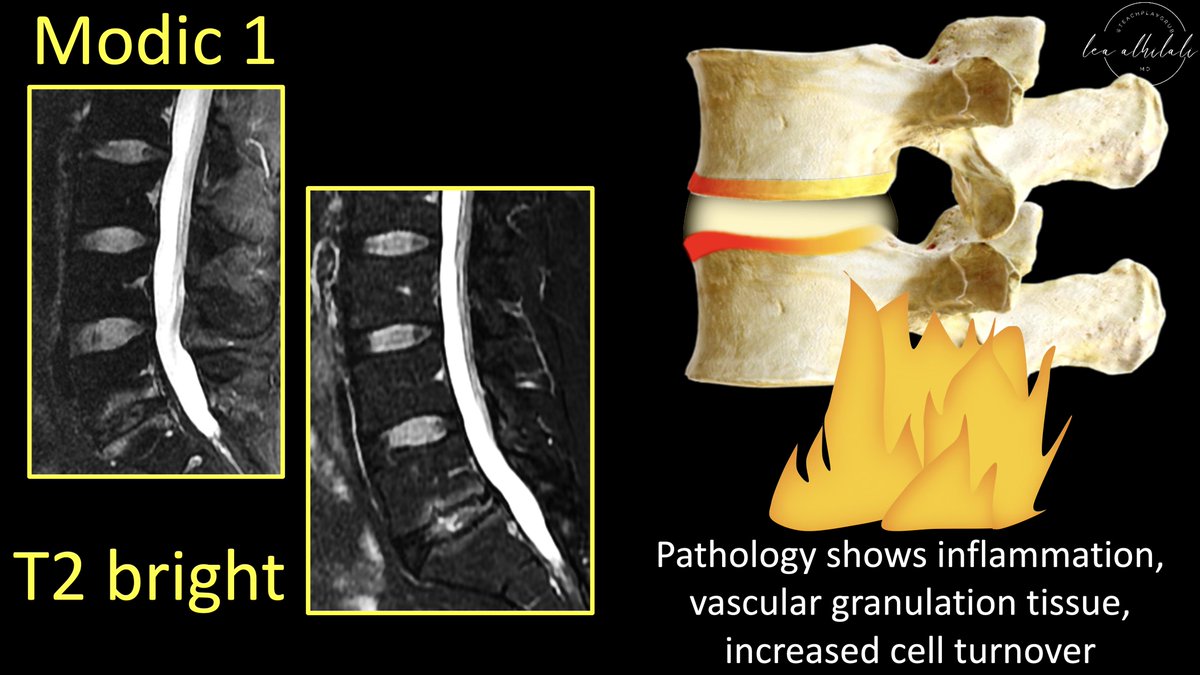
(1) T2 bright changes (indicating edema, Modic 1)
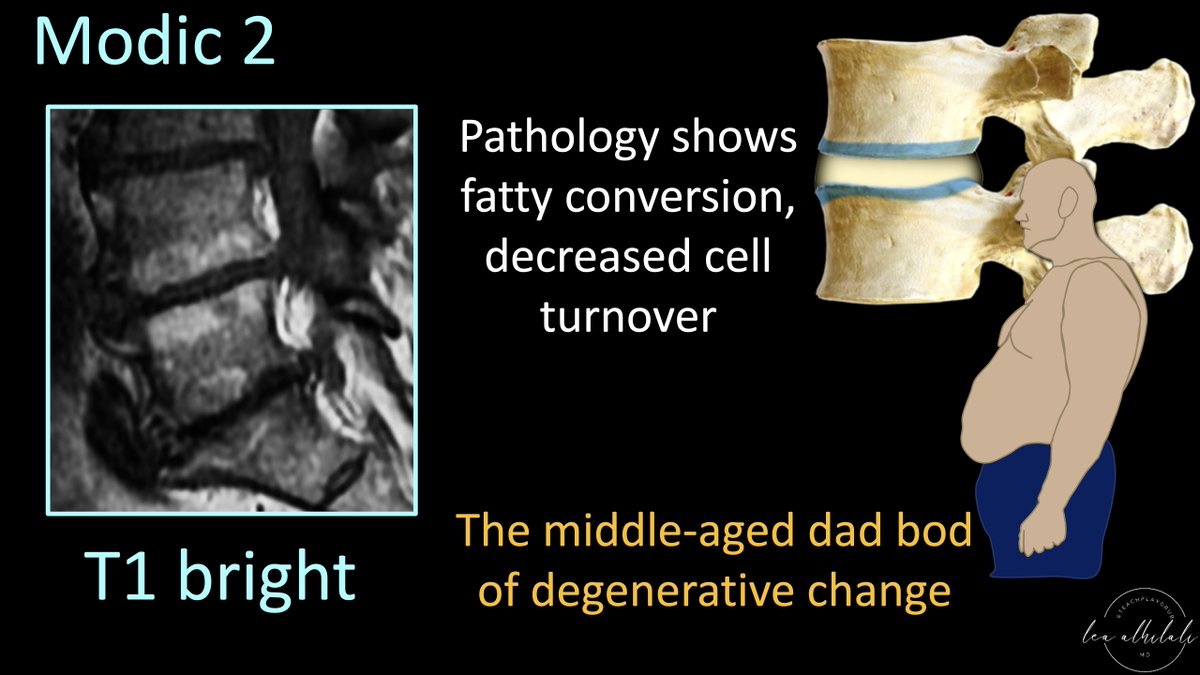
(2) T1 bright changes (indicating fat, Modic 2)
(3) T1 & T2 dark changes (indicating sclerosis, Modic 3)
But what do they mean?
(1) T2 bright changes (indicating edema, Modic 1)
(2) T1 bright changes (indicating fat, Modic 2)
(3) T1 & T2 dark changes (indicating sclerosis, Modic 3)
But what do they mean?

3/Let’s start w/Modic 1.
These are bright on T2, indicating edema
On pathology, it’s what you’d expect w/edema: inflammation, vascular granulation tissue, & high cellular turnover
Vascular granulation tissue means these can enhance on post contrast images—mimicking discitis!
These are bright on T2, indicating edema
On pathology, it’s what you’d expect w/edema: inflammation, vascular granulation tissue, & high cellular turnover
Vascular granulation tissue means these can enhance on post contrast images—mimicking discitis!
4/Modic 2 changes seem to be when the pendulum swings the other direction.
These are bright on T1, indicating fat.
They show fatty conversion of the marrow & low cellular turnover.
I think of them as the middle-aged dad bod of degenerative change—lots of fat & slow to change!
These are bright on T1, indicating fat.
They show fatty conversion of the marrow & low cellular turnover.
I think of them as the middle-aged dad bod of degenerative change—lots of fat & slow to change!
5/Modic 3 changes seem to be the endgame.
These are dark on T1 & T2, indicating sclerosis—which is what you see on pathology: dense fibrous tissue & sclerosis.
It’s like the endplates get fossilized—once you turn into rock, you are never going back.
These are dark on T1 & T2, indicating sclerosis—which is what you see on pathology: dense fibrous tissue & sclerosis.
It’s like the endplates get fossilized—once you turn into rock, you are never going back.

6/I remember these bc the forces at work in the endplates are like the famous astrology signs—almost.
Instead of earth, wind, & fire—it’s earth (sclerosis), fat, & fire (inflammation)
Instead of earth, wind, & fire—it’s earth (sclerosis), fat, & fire (inflammation)

7/Although, it can also be earth, WIND, & fire
Just remember: when we eat a big fatty meal, we tend give off some, well, gas or WIND.
So why is inflammation type 1, fat type 2, and sclerosis type 3?
Just remember: when we eat a big fatty meal, we tend give off some, well, gas or WIND.
So why is inflammation type 1, fat type 2, and sclerosis type 3?

8/Modic watched patients longitudinally & found inflammation turned to fat but never the other way around.
So he hypothesized these are the stepwise chronological changes of the endplates in response to stress & degeneration
They mirror the same way we respond to stress & conflict
So he hypothesized these are the stepwise chronological changes of the endplates in response to stress & degeneration
They mirror the same way we respond to stress & conflict
9/Endplates are like two neighbors w/a wall (disc) separating them.
When the wall is too thin, you get conflict! This is what happens when disc degenerates!
Your first response is anger & yelling at them to keep it down!
Just like the endplates, you first get inflamed
When the wall is too thin, you get conflict! This is what happens when disc degenerates!
Your first response is anger & yelling at them to keep it down!
Just like the endplates, you first get inflamed

10/When anger & inflammation don’t resolve it, you give up, get depressed & start stress eating.
Same w/the endplates! You will transition to from inflammation to low turnover & fat!
Same w/the endplates! You will transition to from inflammation to low turnover & fat!

11/Finally, you try to resolve the conflict by reinforcing the barrier between you by adding some rock
Same w/the endplates. They start to increase the bony sclerosis between them.
Same w/the endplates. They start to increase the bony sclerosis between them.

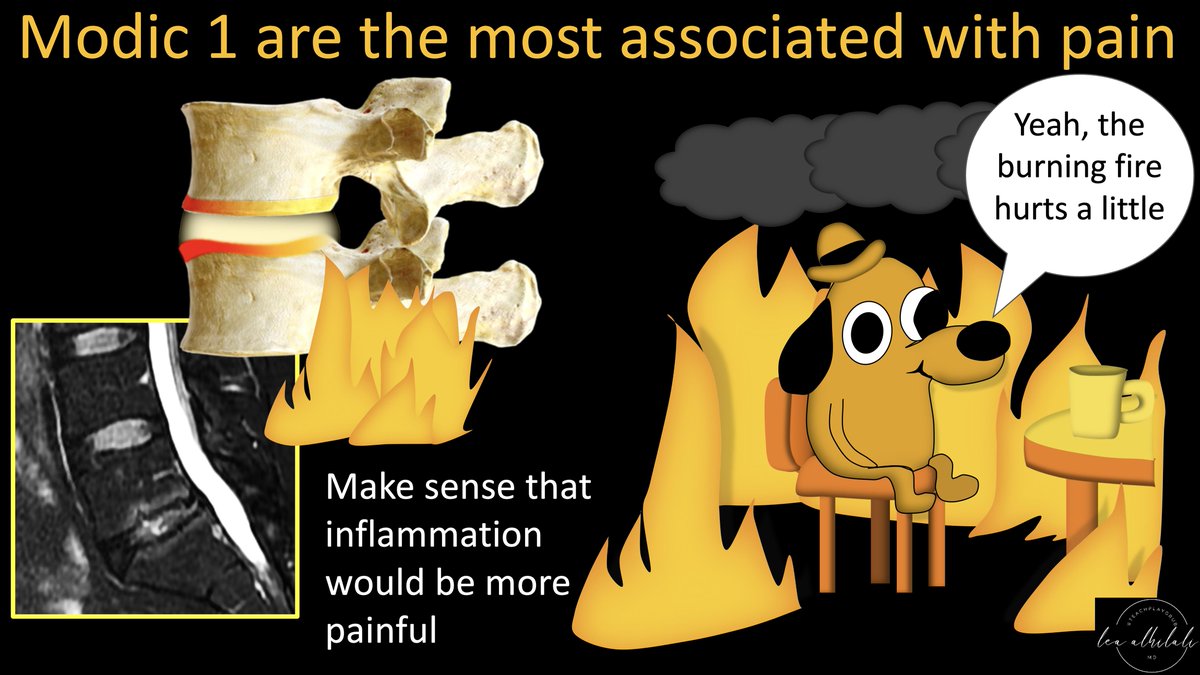
12/But why are degenerative endplate changes important?
Most important reason is that Modic 1 changes are associated w/pain.
It makes sense, as inflammation tends to be painful, as opposed to fatty atrophy.
This pain can sometimes be treated w/basivertebral nerve ablation
Most important reason is that Modic 1 changes are associated w/pain.
It makes sense, as inflammation tends to be painful, as opposed to fatty atrophy.
This pain can sometimes be treated w/basivertebral nerve ablation
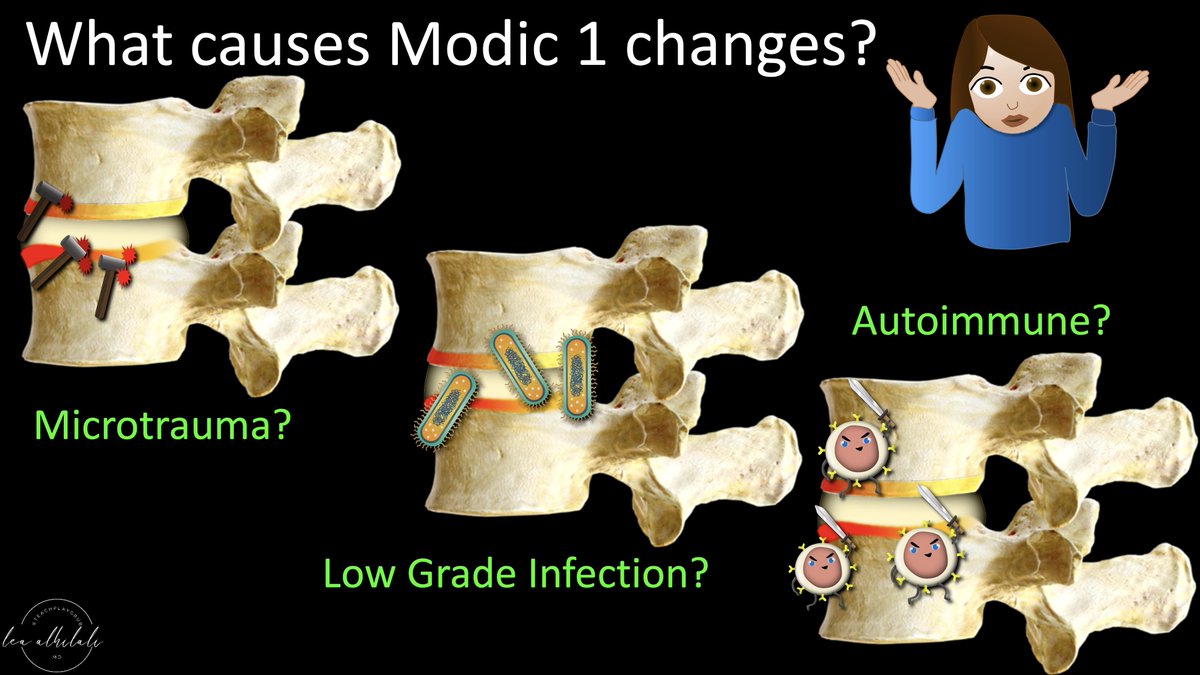
13/So what causes these Modic 1 inflammatory changes?
Sadly, after >30 years, we still don’t really know.
Theories include microtrauma, low grade infection, or an autoimmune response.
Basically, you can remember the things that get YOU inflamed
Sadly, after >30 years, we still don’t really know.
Theories include microtrauma, low grade infection, or an autoimmune response.
Basically, you can remember the things that get YOU inflamed
14/First is microtrauma
Just like little annoyances from a coworker eventually get you inflamed, same happens w/endplates
Microtraumas constantly happens. So there’s a frustrated healing response—bc there’s no break for endplates to fully heal, so you get inflammation
Just like little annoyances from a coworker eventually get you inflamed, same happens w/endplates
Microtraumas constantly happens. So there’s a frustrated healing response—bc there’s no break for endplates to fully heal, so you get inflammation
15/Next is low grade infection
Low grade bacteria have been cultured from Modic 1 changes.
It’s just like how you are more like to get super annoyed when you are already feeling sick!
However, this theory is not widely accepted & many dismiss it.
Low grade bacteria have been cultured from Modic 1 changes.
It’s just like how you are more like to get super annoyed when you are already feeling sick!
However, this theory is not widely accepted & many dismiss it.
16/Finally is autoimmune.
Nucleus pulposis is notochord. It’s shielded from the immune system early in development—meaning the immune system never recognizes it as its own
It’s like having a brother that is separated from you at birth, so you never get to know him
Nucleus pulposis is notochord. It’s shielded from the immune system early in development—meaning the immune system never recognizes it as its own
It’s like having a brother that is separated from you at birth, so you never get to know him
17/When the disc fissures & exposes it, it gets attacked as foreign by the immune system
It’s the same way you would get inflamed if you met your long lost brother. You wouldn’t know him & you would freak out!
It’s the same way you would get inflamed if you met your long lost brother. You wouldn’t know him & you would freak out!
18/So now you know the types of degenerative endplate changes, why their important, & the theories as to why they happen.
Now you can use this when you go BACK to work on reading spine MRIs!
Now you can use this when you go BACK to work on reading spine MRIs!
• • •
Missing some Tweet in this thread? You can try to
force a refresh