
51M & daughter in California admitted w fever/resp failure/hemoptysis. CXR +mutifocal PNA. Father +tender groin LN. Bcx +GNB bipolar staining. Next day, 13 other pts from the same area, admitted w severe PNA. Reported handling dead rats. Recomm isolation precaution on admission?
(1/5) Answer: droplet isolation. The rapidly progressive pneumonia, tender lymphadenopathy (index patient), epidemiologic link to handling dead rodents, the high attack rate, & the bipolar staining GNB seen on blood culture all point to 🌟📌💡plague (Yersinia pestis). #meded
(2/5) When plague is suspected, patients should be placed on 🌟droplet isolation until 48H of effective Rx (1st line: gentamicin). 📌Person-person transmission of plague has only been observed in the pneumonic form. 💡#meded
(3/5) Other forms (often overlapping): bubonic (tender, suppurative LN; 🌟most common), septicemic (no localizing features). Human transmission: 📌flea bite (most common), direct inoculation (handling dead rats), inhalation (pneumonic form, suspect 💡bioterrorism also). #meded
(4/5) Plague endemic areas: sub-Saharan Africa (🌟Madagascar, used as buzzword sometimes in the board exam); in the western US, seen in New Mexico, Arizona, Colorado, California. #meded
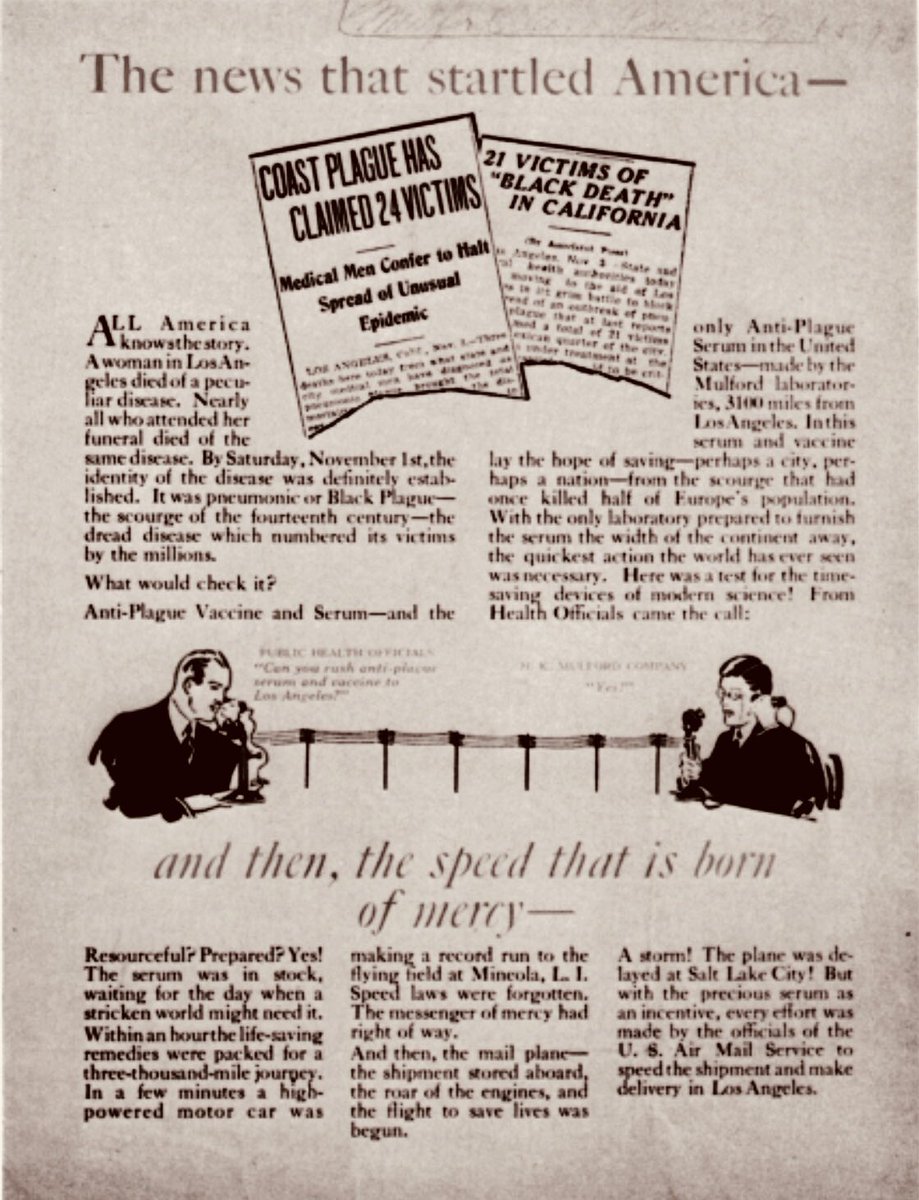
(5/6) #medhistory Holloween of 1924, almost exactly 94 yrs ago, there was an outbreak of plague in Los Angeles. 🌟The case presented in the quiz is actually how this outbreak started in 1924 #historyofmedicine #history #meded. Read more about it here: ncbi.nlm.nih.gov/pmc/articles/P… 
• • •
Missing some Tweet in this thread? You can try to
force a refresh




