62 y/o man, O positive with de novo AML undergoes workup for Hematopoietic Stem Cell Transplant (HSCT). 😃Good news: Sibling with 8/8 HLA match! 👎🏽Bad news: Sibling is A positive. Can this sibling be a donor?
#Blooducation #PathTweetorial #HSCT
#Blooducation #PathTweetorial #HSCT
Unlike solid organ transplants, ABO-mismatch HSCT is not a barrier. In fact, 25-50% of all HSCT are ABO-incompatible. The most important factor in transplant survival outcomes is HLA compatibility (Chrom. 6p)
✅Critical to engraftment
✅ Balances potential harm of GVHD vs GVL
✅Critical to engraftment
✅ Balances potential harm of GVHD vs GVL



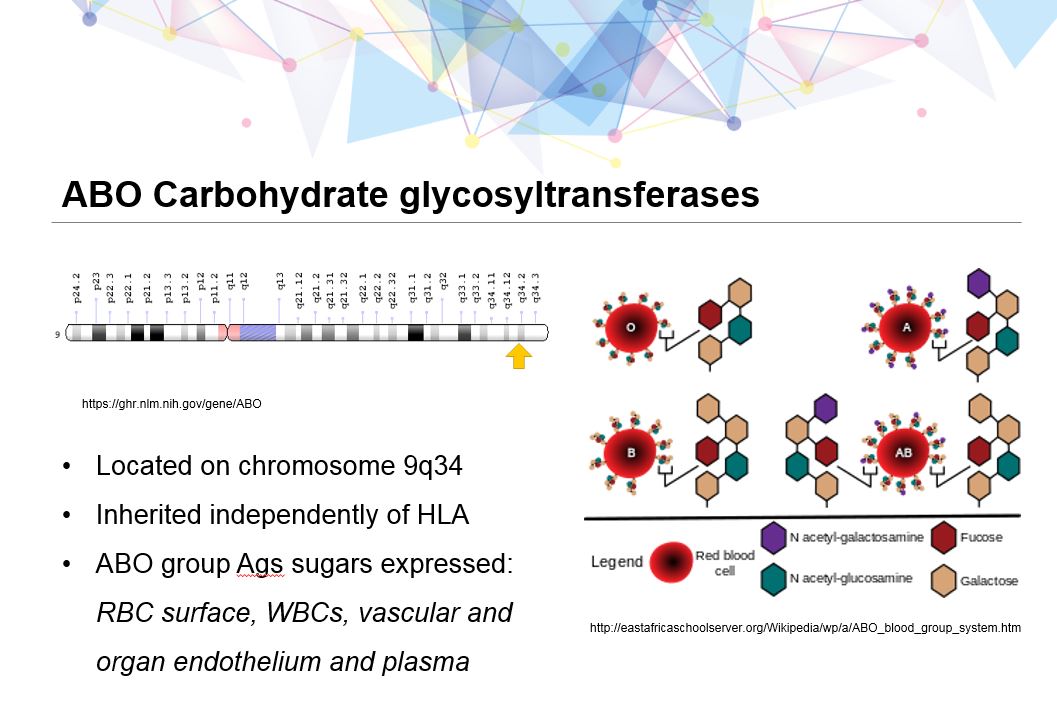
ABO carbohydrate glycosyltransferases are genes located on chromosome 9 and inherited completed independent of HLA. ABO Ags are not only on RBC membranes, but are also expressed on PLTs, vascular and organ endothelium as well as present in the plasma.
#Blooducation
#Blooducation
Based on the patient recipient/donor relationship above, which type of ABO-mismatch exists?
Recipient = O positive, Donor = A positive
Recipient = O positive, Donor = A positive
ABO-mismatch is divided into 3 categories: Major, Minor and Bidirectional.
Ask yourself, where are the dangerous isohemagglutinins (antibodies) that can cause hemolysis– the recipient or donor?
Ask yourself, where are the dangerous isohemagglutinins (antibodies) that can cause hemolysis– the recipient or donor?

Major: Donor – type A, B, or AB/ Recipient – type O, anti-A & anti-B antibodies
💡Recipient has anti-donor antibodies that can cause acute hemolysis of donor RBCs in product
💡Recipient has anti-donor antibodies that can cause acute hemolysis of donor RBCs in product

Minor: Donor – type O, anti-A & anti-B antibodies/ Recipient – type A, B or AB
💡Donor has anti-recipient antibodies that can cause acute hemolysis of recipient RBCs
💡Donor has anti-recipient antibodies that can cause acute hemolysis of recipient RBCs

Bidirectional: Donor – type A, B, AB, anti-A & anti-B antibodies / Recipient – type A, B, AB, anti-A & anti-B antibodies
Mix of both!
Mix of both!

⁉️What total RBC volume could potentially cause acute hemolysis in a transfused product 🅰️🅱️🆎🅾️?
In the blood bank, if a unit has >20-25 ml of RBCs (RBCs, granulocytes, etc), the unit must be crossmatched to prevent an acute hemolytic transfusion reaction. In addition to acute hemolysis, what other consequences can happen with a MAJOR ABO-mismatch HSCT?
Delayed engraftment and PRA are 2 potential consequences of MAJOR ABO-mismatch HSCT. In order to mitigate this affect, red cell depletions using a number of methods are performed if the unit has more than 20-30 mL of RBCs in final collection product. Here's how to remember:

To learn more about ABO-mismatch HSCT, take a look at this MUST-READ article by Dr. Garret Booth doi.org/10.1016/j.bbmt…
🤔Any other experiences or insights to this process? Please add to the dialogue below! Thank you 🙏🏽@BldCancerDoc @AkshaySharmaMD @psharmaMD @KreuterMD
🤔Any other experiences or insights to this process? Please add to the dialogue below! Thank you 🙏🏽@BldCancerDoc @AkshaySharmaMD @psharmaMD @KreuterMD