
Radiation to the prostate for metastatic prostate cancer is now endorsed by NCCN 2019. This topic can be a bit confusing, so here is a tweetorial for residents & community practice #radonc docs (including my #CleClinicCancer colleagues taking oral boards soon). #pcsm 1/21
I recently pieced together some key points on primary prostate RT for M1 for a resident teaching session, which I thought I’d share here. Apologies in advance if any typos or errors in this thread. 2/21
First, some definitions. mCSPC = metastatic castrate sensitive prostate ca. MDT = metastasis directed therapy (surgery or SBRT to all sites). Oligomets = 1-3 or 1-5 mets. 3/21
A caveat: prognosis of N1M0 much better than M1. ADT + RT now “preferred” for N1M0 by NCCN based on non-randomized data such as STAMPEDE. ncbi.nlm.nih.gov/pubmed/25571871
& ncbi.nlm.nih.gov/pubmed/26606329 4/21
& ncbi.nlm.nih.gov/pubmed/26606329 4/21


For N1M0, can also add abiraterone to ADT +/- RT based on STAMPEDE (FFS benefit but not OS benefit for M0). ncbi.nlm.nih.gov/pubmed/28578639 5/21


OK, moving on to newly diagnosed M1 prostate cancer (mCSPC). For decades, ADT alone was primary “SOC” option. NCCN now endorses additional options based on “volume” (aka “metastatic burden”): abiraterone, docetaxel, or prostate RT. 6/21

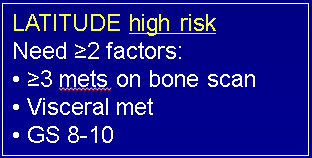
Important to understand differences in “high risk” on LATITUDE and “high volume” on CHAARTED & STAMPEDE trials. Also important to remember that CT, MRI, & bone scans were used to define these (not PET scans!). 7/21

So by CHAARTED/STAMPEDE volume definition, can have multiple pelvic LN+ and innumerable bone mets in spine/pelvis only, and technically still be “low
volume”. This is notably different than “oligometastases” which implies 1-3 or 1-5 mets. 8/21
volume”. This is notably different than “oligometastases” which implies 1-3 or 1-5 mets. 8/21
CHAARTED: adding docetaxel to ADT improved OS for high metastatic burden (HMB) but not low (LMB) mCSPC.
ncbi.nlm.nih.gov/pubmed/26244877 9/21
ncbi.nlm.nih.gov/pubmed/26244877 9/21

STAMPEDE: adding abiraterone to ADT improved OS for both high AND low volume mCSPC. ncbi.nlm.nih.gov/pubmed/28578639
& Hoyle ESMO 2018. 10/21
& Hoyle ESMO 2018. 10/21

So next, STAMPEDE tested “SOC” ADT +/- prostate RT 55 Gy/20 or 36 Gy/6 (weekly) for mCSPC. Note: no LN radiation or MDT given! Also, no abiraterone (18% were planned to get docetaxel as SOC). >2000 pts enrolled! 11/21
STAMPEDE: adding prostate RT to ADT improved OS for pre-specified subset of low volume mCSPC, but NOT for high volume.
ncbi.nlm.nih.gov/pubmed/30355464 12/21
ncbi.nlm.nih.gov/pubmed/30355464 12/21


Similarly, the HORRAD trial randomized mCSPC to ADT +/- prostate RT 70 Gy/35 (or 57.76 Gy/19). Note: no pre-specified volume definition on HORRAD, except # mets on bone scan (<5, 5-15, >15). 13/21
HORRAD found prostate RT for mCSPC <5 bone mets had trend to better OS with similar hazard ratio (0.68) as STAMPEDE. Again, no LN radiation or MDT.
ncbi.nlm.nih.gov/pubmed/30266309 14/21
ncbi.nlm.nih.gov/pubmed/30266309 14/21

STOPCAP meta-analysis combined STAMPEDE & HORRAD data, stratifying by # mets & found prostate RT + ADT improved 3-yr OS by 7% over ADT alone for mCSPC <5 bone mets. ncbi.nlm.nih.gov/pubmed/30826218 15/21

So we now have high level evidence that prostate RT + ADT improves OS over ADT alone for mCPSC by CHAARTED/STAMPEDE low volume definition, or more simply <5 bone mets per STOPCAP. Remember: staging based on CT, MRI, bone scans (not PET). 16/21

NCCN 2019 endorses prostate RT 55 Gy/20 or 36 Gy/6 weekly for low vol mCSPC (no LN radiation or MDT). Prostate RT compared to ADT + abi yet untested (await PEACE-1 trial). For high vol mCSPC, only role of RT is palliation. No role yet for RP in M1 except on trial (SWOG). 17/21

So, how about oligometastatic prostate cancer? Best prospective data comes from STOMP, a randomized phase II trial of MDT (surgery or SBRT) vs. surveillance for 62 pts w/ 1-3 oligomets on choline PET.
ncbi.nlm.nih.gov/pubmed/29240541 18/21
ncbi.nlm.nih.gov/pubmed/29240541 18/21
STOMP: all patients were asymptomatic & oligo-recurrent (on choline PET) after previous treatment to prostate. This is a VERY different population than in the aforementioned newly diagnosed mCSPC trials. 19/21
Per STOMP, MDT may prolong ADT-free survival w/ acceptable toxicity, but more trials like ORIOLE are needed to study MDT for prostate cancer oligomets (SABR-COMET enrolled only 16 prostate ca pts). 20/21

In summary, prostate RT + ADT for low vol mCSPC (by CHAARTED/STAMPEDE defn or <5 bone mets per STOPCAP) improves OS even without LN radiation or MDT. Amazing work by @Prof_Nick_James, @PCaParker, @piet_ost et al! 21/21
P.S. and PET scans, when they become ubiquitous, will change *everything* that we know so far.
@threadreaderapp unroll please
• • •
Missing some Tweet in this thread? You can try to
force a refresh


