Quick Tutorial Thread for Twitter
Psychiatric Cardiology 101: QTc
Wherein a psychiatrist tries to teach cardiology (and hopefully doesn't embarrass themselves)
#psychtwitter #medtwitter #MedEd #psychchat #somemed #somepsych
Warning: MATH
Psychiatric Cardiology 101: QTc
Wherein a psychiatrist tries to teach cardiology (and hopefully doesn't embarrass themselves)
#psychtwitter #medtwitter #MedEd #psychchat #somemed #somepsych
Warning: MATH
What is QT? (Yes yes, it can be your texting shorthand to get your groove on)
QT refers to the interval on the electrocardiocgram, in milliseconds, between the START of the QRS complex to the END of the T Wave
QT refers to the interval on the electrocardiocgram, in milliseconds, between the START of the QRS complex to the END of the T Wave

(as the graph shows, if you wanna be super fancy, we calculate the end of the T wave by intersecting the maximum slope with the isoelectric baseline)
Why is QT important?
It is the electrical approximation of the time it takes for the ventricles to contract and relax
If the QT is too long (or short, think hypercalcemia and be careful, but we'll address this later), there is a risk for ventricular dysthymia and sudden death.
It is the electrical approximation of the time it takes for the ventricles to contract and relax
If the QT is too long (or short, think hypercalcemia and be careful, but we'll address this later), there is a risk for ventricular dysthymia and sudden death.
Long QT can lead to Torsades de Pointes (literally "twisting of the peaks"), which looks like a ventricular tachycardia rotating (like a helix).
TdP spontaneously and quickly reverts to normal rhythm, but it is likely to return & can lead to ventricular fibrillation and death.
TdP spontaneously and quickly reverts to normal rhythm, but it is likely to return & can lead to ventricular fibrillation and death.

So then what is QTc?
Well because rate will affect all intervals, it is necessary to adjust for rate to detect clinically important QT. With a fast rate, a shorter QT might be important, so you don't want to miss it. Conversely, you can tolerate longer QTs with a slow rate.
Well because rate will affect all intervals, it is necessary to adjust for rate to detect clinically important QT. With a fast rate, a shorter QT might be important, so you don't want to miss it. Conversely, you can tolerate longer QTs with a slow rate.
QTc is calculated by three main formulas. There is debate over which is best... but most of the cardiologists I respect tell me the Frederica formula is probably the closest.
1) calculate: RR interval in seconds
2) cube root that
3) use that number as the divisor of the QT
1) calculate: RR interval in seconds
2) cube root that
3) use that number as the divisor of the QT

Example:
HR is 80bpm (RR = 60/HR = 0.75)
QT is 425msec
The cube root of RR is .9086
QTc=425msec/.9086=468 msec
HR is 80bpm (RR = 60/HR = 0.75)
QT is 425msec
The cube root of RR is .9086
QTc=425msec/.9086=468 msec
So you have your QTc, now what?
1) please do your best to understand how your QTc will be calculated. Many machines that calculate it automatically will give you the Bazetts Formula (square root not cube root), which overcalls prolonged QTc at faster rates.
1) please do your best to understand how your QTc will be calculated. Many machines that calculate it automatically will give you the Bazetts Formula (square root not cube root), which overcalls prolonged QTc at faster rates.
2) have your yellow/red zone set:
♀️:
caution: 450-460 msec
uh-oh: 460+
♂️:
caution: 430-450 msec
uh-oh: 450+
♀️:
caution: 450-460 msec
uh-oh: 460+
♂️:
caution: 430-450 msec
uh-oh: 450+
3) know your medications effect on QT!
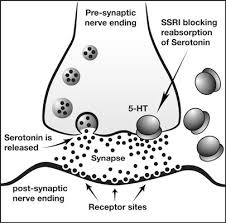
The most FAMOUS psychiatric meds that prolong QT are antidepressants, but MOST DO NOT (except citalopram, escitalopram, and TCAs like amitriptyline)
The most FAMOUS psychiatric meds that prolong QT are antidepressants, but MOST DO NOT (except citalopram, escitalopram, and TCAs like amitriptyline)

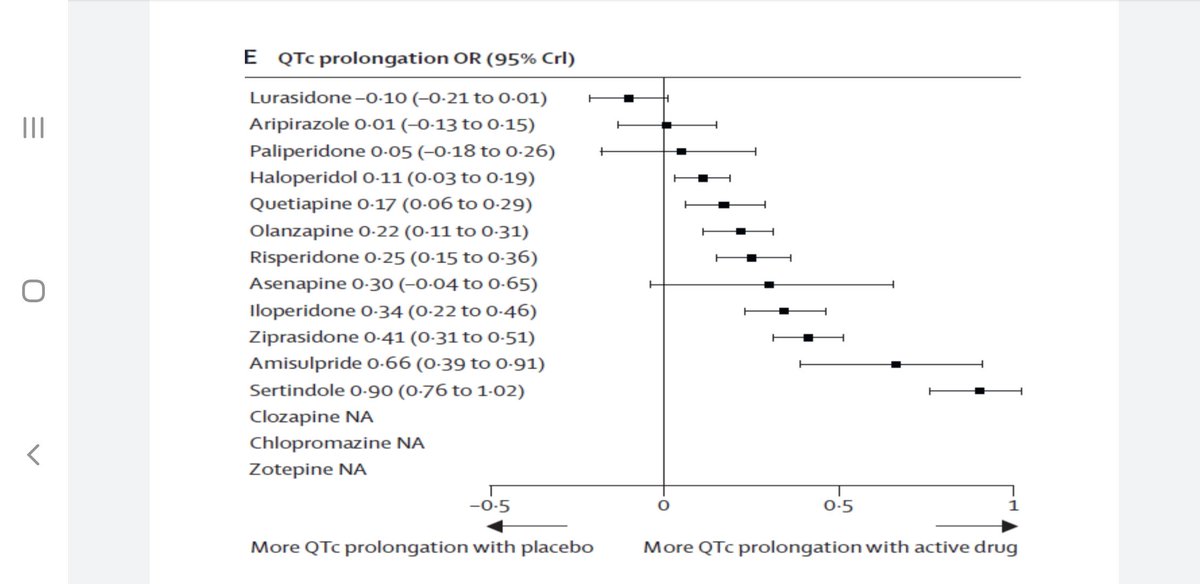
The meds you need to be really careful about? ANTIPSYCHOTICS AND METHADONE. (No, not ADHD meds)
Lurasidone is so far the only "OK" antipsychotic for QT prolongation.
Methadone can increase QTc by more than 20s.
Lurasidone is so far the only "OK" antipsychotic for QT prolongation.
Methadone can increase QTc by more than 20s.
So ECG for all potential QT starts (*citalopram, TCAs, APs)?
I'm on team "yes." It's far higher value than the stupid MRIs and TSHs we order (brainlessly w/no benefit) and if a problem occurs, having a baseline ECG will be of huge value.
I'd also monitor regularly anyone who:
I'm on team "yes." It's far higher value than the stupid MRIs and TSHs we order (brainlessly w/no benefit) and if a problem occurs, having a baseline ECG will be of huge value.
I'd also monitor regularly anyone who:

So please , learners, physicians, and psychiatrists, consider QTc knowledge as an important part of your medical practice, especially when you prescribe medications.
Also, when in doubt, work with your pharmacy colleagues to check interactions/additive effects.
/End thread
Also, when in doubt, work with your pharmacy colleagues to check interactions/additive effects.
/End thread
• • •
Missing some Tweet in this thread? You can try to
force a refresh