HIV. Sickle cell pain crisis. Metabolic acidosis and hypokalemia. 🥼⚕️Just another night on call. Let's break it down in the inaugural #tweetorial by the #FOAMED #medtwitter @TheSkeletonKG
Full post here! @RenalFellowNtwk renalfellow.org/2019/10/03/the…
Full post here! @RenalFellowNtwk renalfellow.org/2019/10/03/the…

30 yo woman with sickle cell anemia and HIV on lamivudine, tenofovir, alafenamide, and efavirenz presents with a pain crisis. 💉💉Labs are shown.

What should we do next?
ABG is as follows. The low pH is consistent with metabolic acidosis. The next step is to further characterize the metabolic acidosis.

1⃣First with Winter's Formula ➡️(pCO2 = 1.5 x HCO3 + 8 ±2) is used to see if there is appropriate respiratory compensation. So (1.5 x 15) + 8 is a predicted pCO2 of 31 ±2.
➡️The actual pCO2 of 30 is within predicted indicating appropriate compensation. 👏
➡️The actual pCO2 of 30 is within predicted indicating appropriate compensation. 👏
2⃣Second with the anion gap➡️(anion gap = Na - Cl - HCO3).
Her anion gap is 10 consistent with a normal-anion gap metabolic acidosis (#NAGMA)
Also, her delta anion gap to delta HCO3 is less than 0.4 (ie pure NAGMA)
Her anion gap is 10 consistent with a normal-anion gap metabolic acidosis (#NAGMA)
Also, her delta anion gap to delta HCO3 is less than 0.4 (ie pure NAGMA)
My favorite 😍 #mnemonic for NAGMA is:
The patient has no diarrhea or gastrointestinal fistula, so we consider a renal etiology for her #NAGMA.
How do we confirm this? With urine studies. #urinetotherescue
How do we confirm this? With urine studies. #urinetotherescue
Her urine studies are as follows.
Urine anion gap ➡️ UrNa + UrK = UrCl = 130 + 42 - 94 = 78
⚡️neGUTive results = likely GI (ie gut) issue
⚡️positive = impaired renal handling of acid
❓What about urine osmolar gap? Read the post!
renalfellow.org/2019/10/03/the…
Urine anion gap ➡️ UrNa + UrK = UrCl = 130 + 42 - 94 = 78
⚡️neGUTive results = likely GI (ie gut) issue
⚡️positive = impaired renal handling of acid
❓What about urine osmolar gap? Read the post!
renalfellow.org/2019/10/03/the…

So, what does it mean?
In acidosis the kidney kicks out extra acid as NH4+ which pairs with Cl-. Negative UAG implies the presence of an unmeasured cation (ie NH4+). This means the kidney is doing its job, so the acidosis is a gut issue.
In acidosis the kidney kicks out extra acid as NH4+ which pairs with Cl-. Negative UAG implies the presence of an unmeasured cation (ie NH4+). This means the kidney is doing its job, so the acidosis is a gut issue.

Now we know our patient has an RTA.
😳How do we differentiate between distal RTA (type 1), proximal RTA (type 2), and hyperkalemic RTA (type 4)?
😳How do we differentiate between distal RTA (type 1), proximal RTA (type 2), and hyperkalemic RTA (type 4)?
📌Hyperkalemic RTA is related to hyporeninemic hypoaldosteronism
📌Proximal RTA prevents the proximal tubule from fully reabsorbing filtered HCO3 (decreasing Tm for HCO3)
📌Distal RTA is a defect in H+ secretion which inhibits generation of new HCO3
📌Proximal RTA prevents the proximal tubule from fully reabsorbing filtered HCO3 (decreasing Tm for HCO3)
📌Distal RTA is a defect in H+ secretion which inhibits generation of new HCO3
The high urine pH means the urine is relatively basic in a patient with an acidosis.
This is consistent with impaired acid secretion…a distal RTA! 🥳🥳🥳🥳
This is consistent with impaired acid secretion…a distal RTA! 🥳🥳🥳🥳

Distal RTA is associated with sickle cell disease through various proposed mechanisms🧐 which are further described here:
jamanetwork.com/journals/jamai…
cjasn.asnjournals.org/content/10/2/3…
It is primarily due to downregulation of the⬇️H+ ATPase in the alpha intercalated cell.
jamanetwork.com/journals/jamai…
cjasn.asnjournals.org/content/10/2/3…
It is primarily due to downregulation of the⬇️H+ ATPase in the alpha intercalated cell.
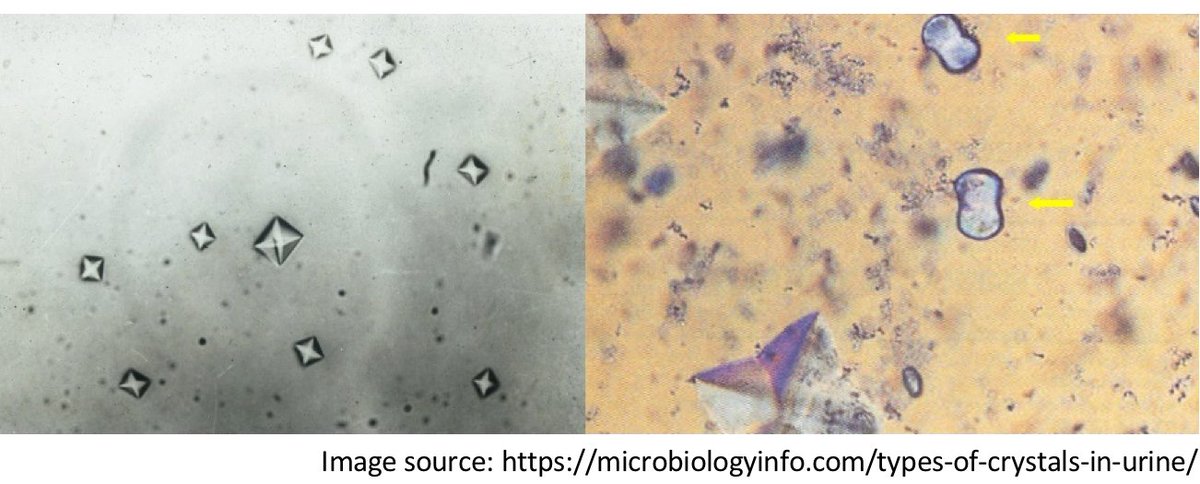
What is the main mechanism for nephrocalcinosis in distal RTA?
Nephrocalcinosis is promoted by the ⬆️high urine pH predisposing to calcium phosphate deposition💎💎

❓But wait…what about her glucosuria and proteinuria??? The collecting duct has nothing to do with those; the proximal tubule is supposed to reabsorb that stuff.🤔
What is causing her proximal tubulopathy?
Summary:
⚡️tenofovir causes proximal tubule damage
⚡️ urine anion gaps indicate appropriate or inappropriate renal handling of ammonium (ie acid)
⚡️ distal RTA have a high urine pH and are associated with nephrocalcinosis
⚡️tenofovir causes proximal tubule damage
⚡️ urine anion gaps indicate appropriate or inappropriate renal handling of ammonium (ie acid)
⚡️ distal RTA have a high urine pH and are associated with nephrocalcinosis
Read the full post and discussion here:
renalfellow.org/2019/10/03/the…
Special thanks to @kidney_boy @SaynaNorouzi
Case author @prakashneph
Editing co-fellows @hotsaltrocks @eljosemenap @christhero10 @drM_sudha @mrcortti_maria @NephroGuy
renalfellow.org/2019/10/03/the…
Special thanks to @kidney_boy @SaynaNorouzi
Case author @prakashneph
Editing co-fellows @hotsaltrocks @eljosemenap @christhero10 @drM_sudha @mrcortti_maria @NephroGuy
• • •
Missing some Tweet in this thread? You can try to
force a refresh