
Can we achieve similar outcomes for lung #SABR in non-academic institutions compared to the major academic centres? This was an important question posed by @drdavidpalma Suresh Senan & @FJLagerwaard. This is a tweetorial to help answer that question. #lcsm #radonc 
The cancer centre in Middlesbrough, is a non-academic #NHS institution serving a regional population of 1.1m. It’s one of the most socially deprived areas in the UK. We started lung SABR in 2009 and presented our long term outcomes at @SABRconsortium 2019 meeting #lcsm #radonc
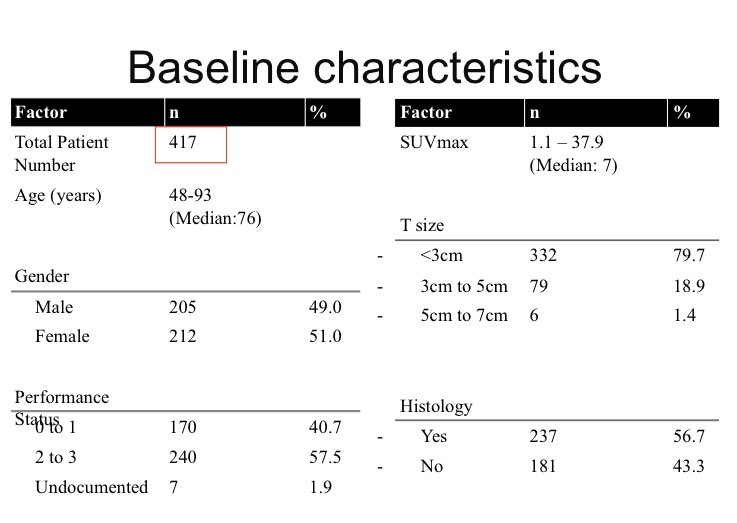
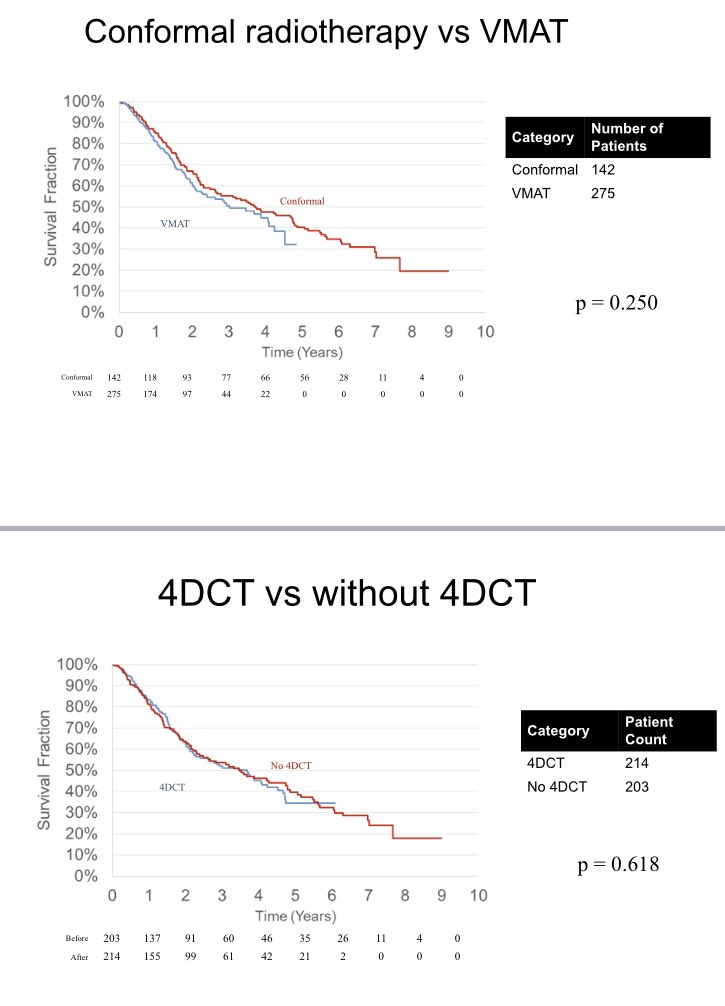
We treated 417 patients over a 10 yr period. SABR technique changed over this time. We introduced 4DCT in 2013 & VMAT in 2014. Prior to this we used a “composite inspiratory/expiratory CT merge” approach, and a 7-field co-planar plans. Doses 54/3, 55/5, 60/8, 50/10 #lcsm #radonc
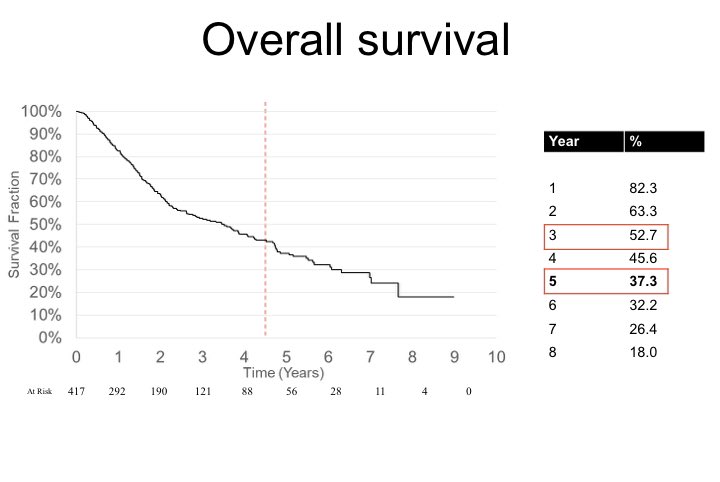
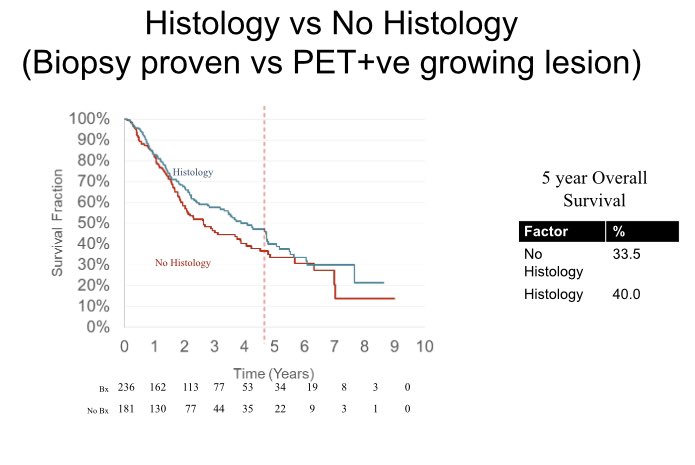
Overall survival results are as follows, which compare really nicely with Timmerman’s RTOG 0236 trial. #LCSM #Radonc
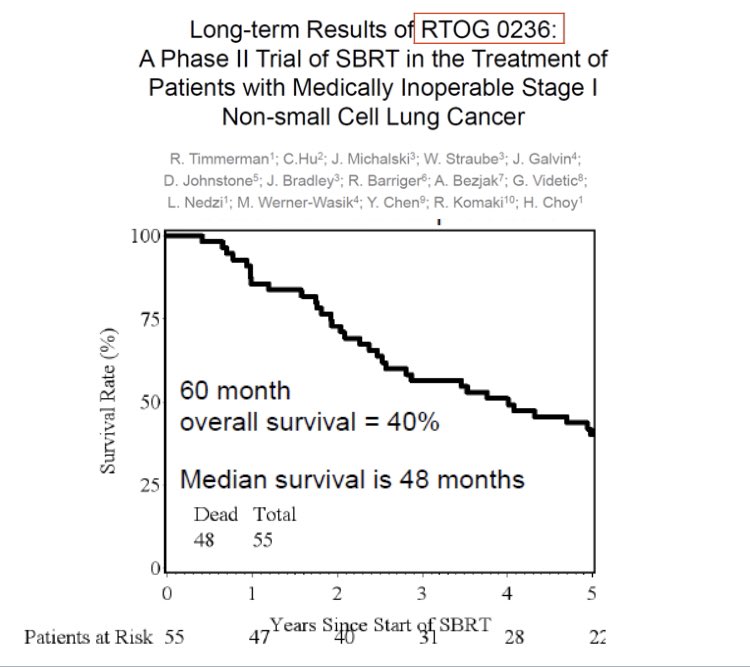
But remember, 100% of the RTOG 0236 patients were biopsy proven NSCLC, so when you compare to our histology positive patients, we match Bob’s results with 40% 5 year survival. #lcsm #radonc
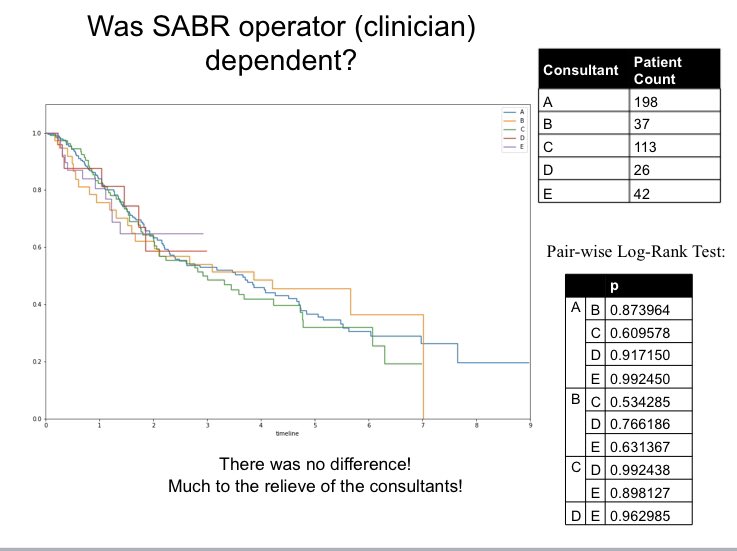
We also looked at whether clinical experience mattered by comparing outcomes between the different consultants - it didn’t. #lcsm #radonc
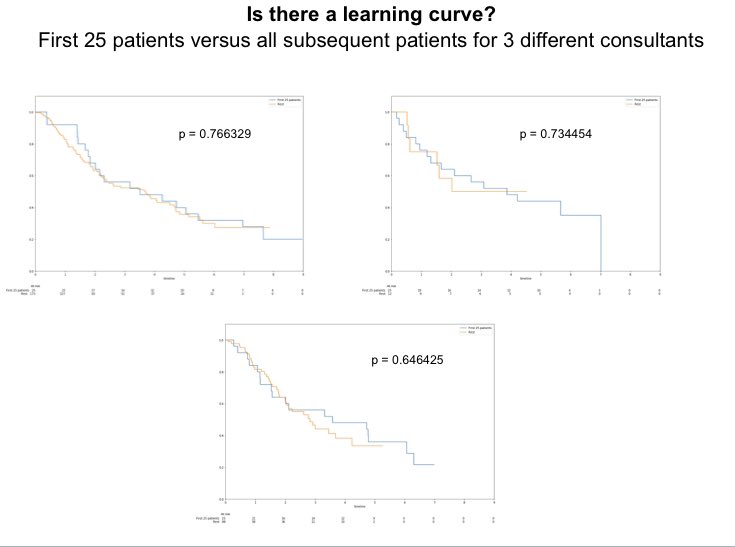
We also looked at whether there was a “learning curve” with a crude measure of looking the first 25 patients treated compared to all subsequent patients (for 3 of the consultants who had done enough cases to make comparison). No apparent learning curve #LCSM #radonc
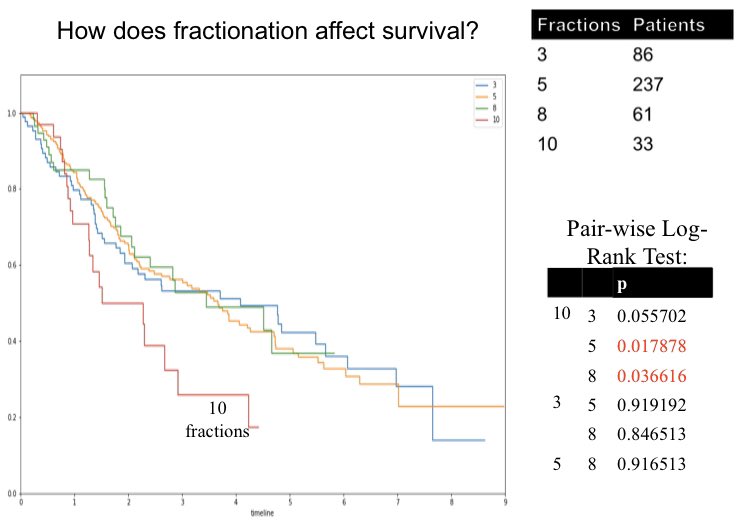
We also compared the different risk-adapted fractionation schedules and 50/10 did badly. No difference between 3, 5, and 8 fractions, though. This supports the >100Gy BED hypothesis. #lcsm #radonc
We then looked at whether new technology like 4DCT and VMAT made a difference to overall survival outcomes - nope! We accept obvious caveat of selection bias during different treatment eras of course. #radonc #lcsm
Bottom line is that lung #SABR to early stage NSCLC can be safely delivered in the non-academic setting with comparable results to major academic institutions. However, training in the technique is essential. Use of @SABRconsortium guidelines & @RTTQA_UK guidance also key #radonc
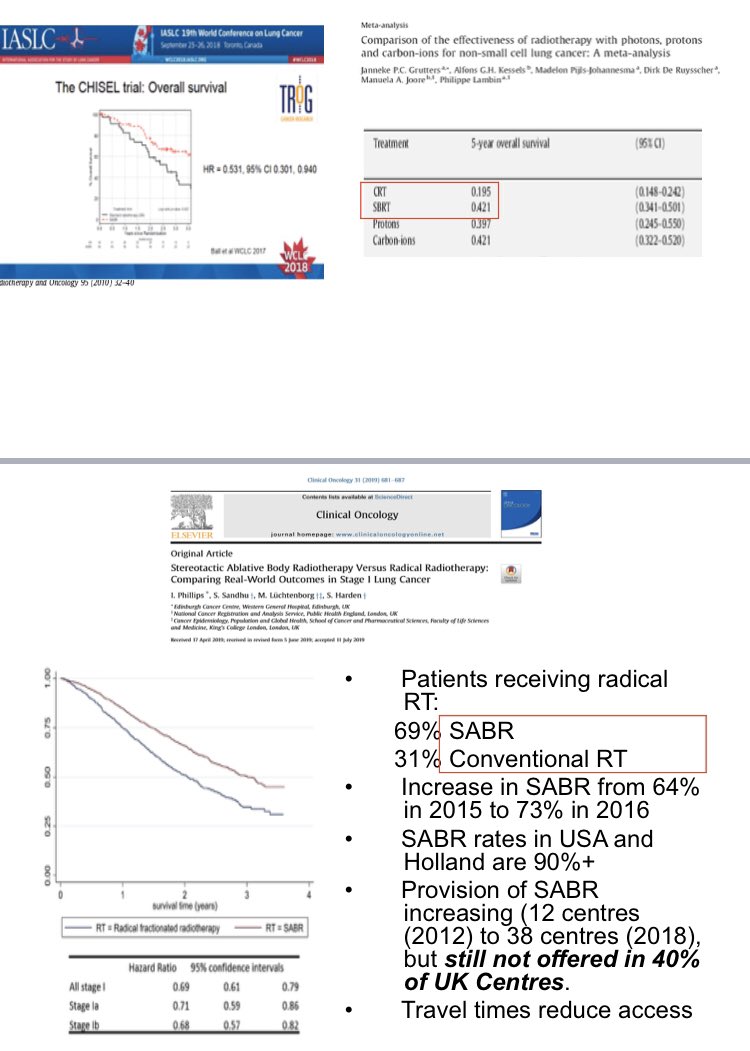
All UK radiotherapy institutions should be allowed to offer lung #SABR with appropriate training. “Buddying” with more experienced centres can help achieve this. With level one evidence showing superiority of SABR over conventional RT, there is no longer any excuse #LCSM #radonc
We have submitted our work to the All Party Parliamentary Group on Radiotherapy who have used it to support the roll out of SABR to all UK radiotherapy centres.
We also believe that although IGRT capability is essential, 4DCT & VMAT are “desirable” rather than crucial. This has important implications for countries around the world with less access to technology. With OS curves like this, getting SABR is more important than “perfect SABR”
Finally, thanks to Dr Alex Wood, a medical student who did his elective with me and put all the data together earlier this year. He’s now qualified and working on the #NHS frontline. Thanks to all the SABR team in the ‘Boro too! #radonc #lcsm
Happy to answer any questions...
Happy to answer any questions...
• • •
Missing some Tweet in this thread? You can try to
force a refresh



