How do you set up pulse pressure variation (PPV) on the monitor? This, of course, requires an arterial line.
Here, @lillieannamd #CleClinicRespiratory shows us how it's done, quickly, on a Phillips monitor. After, we'll talk about uses wrt preload responsiveness... #tweetorial
Here, @lillieannamd #CleClinicRespiratory shows us how it's done, quickly, on a Phillips monitor. After, we'll talk about uses wrt preload responsiveness... #tweetorial
PPV leverages the changes in preload owing to mechanical ventilation, effectively testing where the pt is on the starling curve. A positive response (threshold 12%) suggests they are on a dynamic portion of the curve. 

There are key assumptions which must be met for this to be valid. Namely:
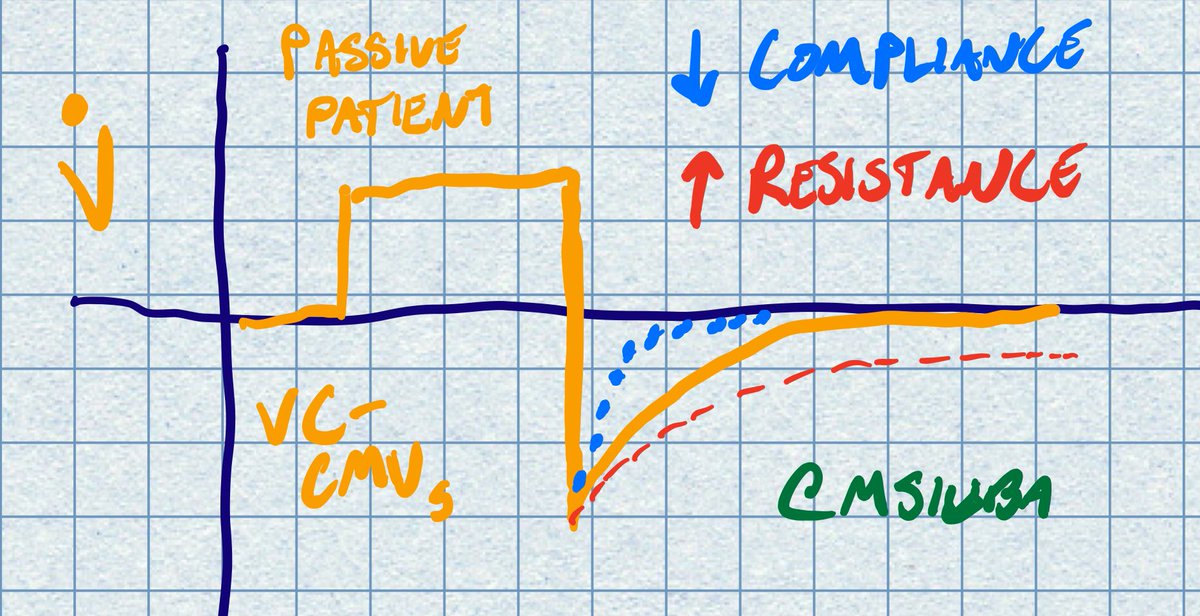
(1) Patient must be PASSIVELY mechanically ventilated
(2) In sinus rhythm
(3) Tidal volume 8-10 ml/kg.
Key ref: annalsofintensivecare.springeropen.com/articles/10.11…
(1) Patient must be PASSIVELY mechanically ventilated
(2) In sinus rhythm
(3) Tidal volume 8-10 ml/kg.
Key ref: annalsofintensivecare.springeropen.com/articles/10.11…
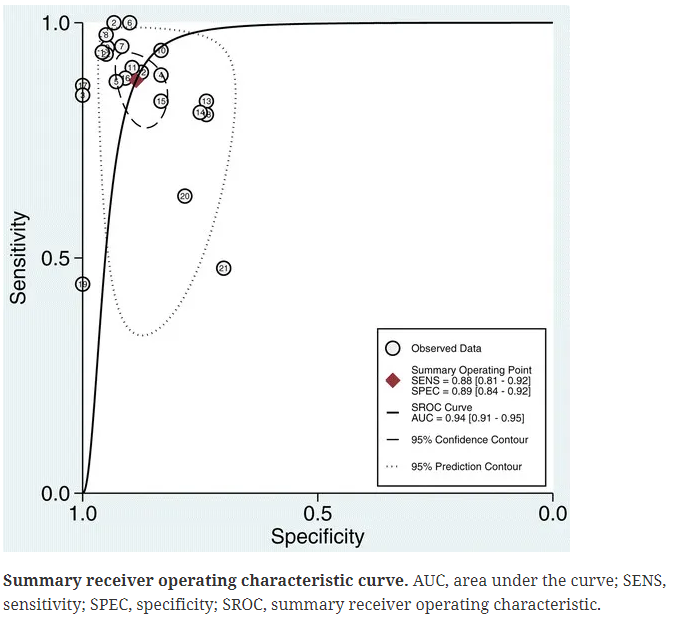
Under these circumstances, the test characteristics are excellent! ROC AUC 0.94 (95% CI 0.91 to 0.95).
Key ref: ccforum.biomedcentral.com/articles/10.11…
Key ref: ccforum.biomedcentral.com/articles/10.11…
Unfortunately, the required assumptions are only met ~17% of the time (doi.org/10.1016%2Fj.ac…)
Also, many times the operators are unaware of the assumptions & possible pitfalls! (doi.org/10.1016%2Fj.ac…)
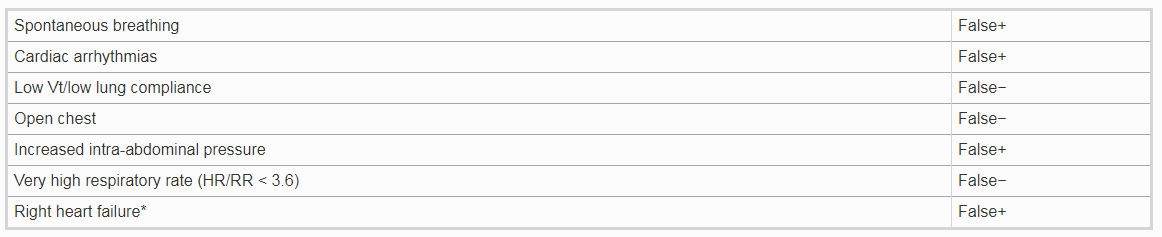
Here are some additional parameters which can threaten interpretation:
Also, many times the operators are unaware of the assumptions & possible pitfalls! (doi.org/10.1016%2Fj.ac…)
Here are some additional parameters which can threaten interpretation:
As with any other test, we should also carefully consider the pretest probability. Look at my favorite graph from ANDROMEDA-SHOCK showing change in preload responsiveness over only *8* hours!

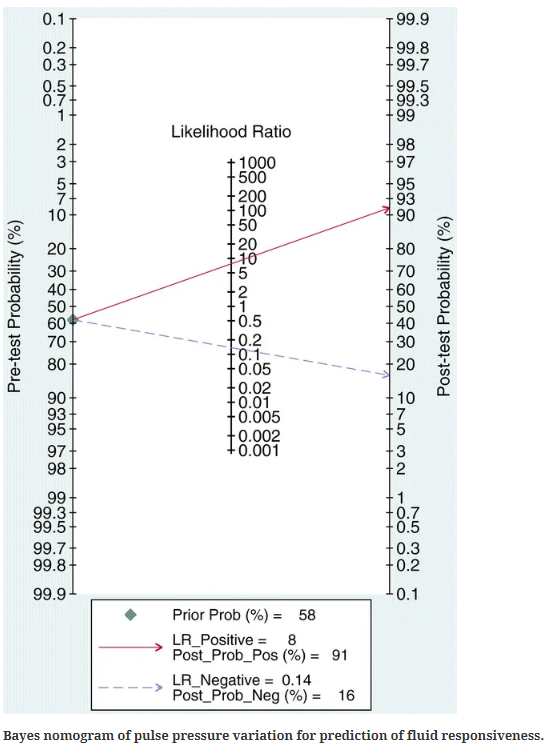
And here's an example using LRs assuming a 60% pretest prob of preload response, and how your posterior would line up based on results
Based on pretest probability over time, I spend a lot of time using PPV to talk people *out* of giving volume! It's a much easier test than e.g. LVOT VTI as the results are displayed continuously. Biggest adjustment you might have to make is increased tidal volume for a few min.
What if the PPV is positive? Should I give volume until I obliterate it? This is a data-sparse zone.
My argument is NO, as that would seem to create a pathologic state on the flat portion of the curve.
Furthermore, there are no hard outcomes a/w treating preload response.
My argument is NO, as that would seem to create a pathologic state on the flat portion of the curve.
Furthermore, there are no hard outcomes a/w treating preload response.

We *do* know that positive fluid balance is associated with mortality and other negative outcomes in the critically ill. So tread lightly. And as @PulmCrit has suggested, make sure you are meeting some sort of physiologic endpoint if you decide to bolus.
emcrit.org/pulmcrit/bolus/
emcrit.org/pulmcrit/bolus/
In summary:
- PPV is useful for preload responsiveness (if appropriate criteria are met)
- Pretest prob of responsiveness is intermediate at best, and diminishes over time (hours!)
- Like many #zentensivist practices, less is more. Be cautious with fluid administration!
- PPV is useful for preload responsiveness (if appropriate criteria are met)
- Pretest prob of responsiveness is intermediate at best, and diminishes over time (hours!)
- Like many #zentensivist practices, less is more. Be cautious with fluid administration!
@threadreaderapp unroll please