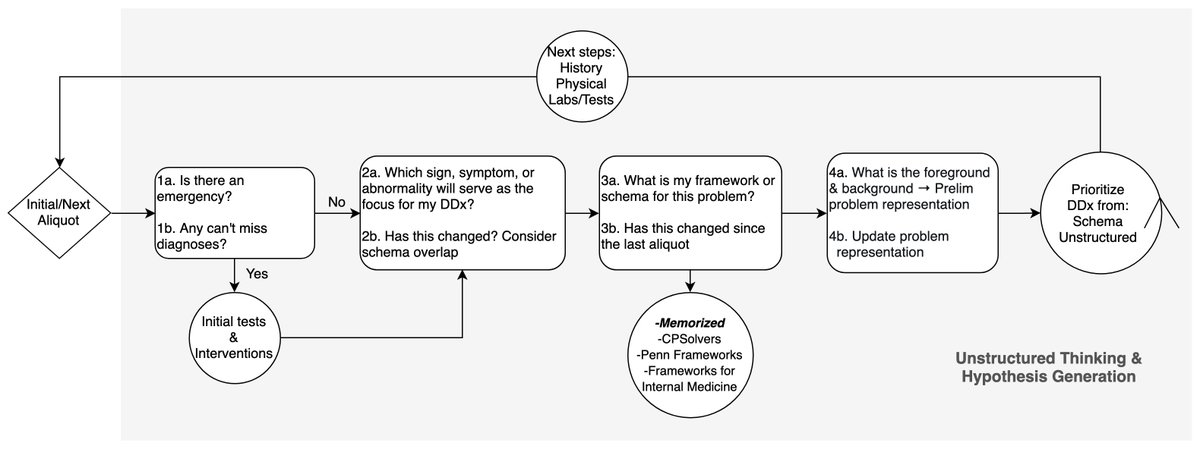
@sargsyanz @hdx @NEJM Thank you, this is amazing! Updated version: gray shaded area represents the space of unstructured thinking, thanks @gradydoctor @HannahRAbrams @Anand_88_Patel for chiming in, your edits been so helpful in thinking about the nuanced ways we approach cases 🙏🏾 
• • •
Missing some Tweet in this thread? You can try to
force a refresh