
Information regarding CO2 insufflation in laparoscopy and robotics has been murky, overwhelming, and confusing. I put together this tweetorial to distill down the information into one thread. To be clear, most info is speculative and extrapolated (ncbi.nlm.nih.gov/pubmed/32221118)
To start, some basic virology needs to be explained. Coronaviruses are a family RNA viruses. The one we’re dealing with today has been named Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) aka coronavirus disease 2019 (i.e., #COVID19).
This RNA virus has a size range of 0.06 to 0.14 microns (ncbi.nlm.nih.gov/pubmed/31978945) and has been isolated within the epithelium of both the respiratory and GI tract. We don’t yet know if it can be isolated within the peritoneal surface or ascitic fluid, but studies are underway.
Studies have also shown that virus may be aerosolized by cauterizing tissue that is infected with many viruses, including HPV, HIV, and HepB, etc (ncbi.nlm.nih.gov/pubmed/16002179). COVID-19 hasn’t been studied yet specifically but the concept of aerosolization is sound nonetheless.
Herein lies the dilemma: (1) prevention of aerosolization, and (2) prevention of transmission.
First, to prevent aerosolization, societies have advocated simply not operating unless absolutely mandatory, eliminate use of energy devices altogether, or at least at their absolute lowest settings. (facs.org/covid-19; sages.org/category/covid…; eaes.eu/category/covid…)
Second dilemma, prevent transmission. For this we’re just assuming that aerosolization is a fact of life, and we need to minimize/prevent transmission. This is where filtration and masks come in.
Let's start with filtration... As for lap/robotic cases that require CO2 insufflation, and depending on the device you're using, filtration occurs during the entirety of the case.
Knowing the viral particle size ranges from 0.06-0.14 microns (see above), the scary issue arises if improperly sized filters are present.
This means that during the case, CO2 enters in via an inflow cannula and either the CO2 remains trapped intraabdominally (along with aerosolized virus), or it is recirculated through the insufflator, filtered, then exhausted through the back of the insufflator as room air.
If a CO2 insufflation filter too large to capture the smaller RNA viral particles is being used in that case, aerosolized viral particles are essentially being concentrated within the exhaust and then expelled out of rear of the insufflator.
Proper CO2 filtration is critical. Only 2 insufflators are commercially available that filter viral particles in the range of COVID-19. Those are @ConMedAirSeal (which filters down to 0.01 micron) bit.ly/34uourX) ...
... and Stryker’s Pnemoclear (which filters down to 0.05 microns) (bit.ly/2XF1ZPZ). That’s it. There aren’t any other insufflators that will adequately filter down to the size the COVID-19 exists to mitigate this potential threat.
But one more point of clarification regarding Air Seal. There are 2 different devices that they sell.
The trifurcated tube set (which is the one we all have that uses an Air Seal valveless trocar, the ASM-EVAC [first pic]) and the bifurcated tube set (which attaches to two standard ports [the SEM-EVAC (the second pic)]). 


To be clear -- the ASM-EVAC can, but should NOT be used! Its valveless port allows CO2 to escape throughout the case if the intraabdominal pressure ever rises too high, or during instrument exchange, etc. This is called an open loop and should be avoided.

@ConMedAirSeal published suggested mitigation strategies by using constant negative pressure smoke evacuators on other valved ports to be placed on suction, but this doesn’t stop valveless trocar leak, it only tries to minimize it. Only the (closed loop) SEM-EVAC should be used.

The second commercially available insufflator is the Stryker Pneumoclear.

The PneumoClear Tube Set is comprised of a series of filters: 1 absorbent layer, 1 ULPA filter, 1 PVDF filter, and 2 charcoal layers. These tube sets filter particles as small as 0.051 microns with up to 99.999993% efficiency for outflow (sages.org/wp-content/upl…).




#funfact: HEPA filters can remove up to 99.97% of contaminants as small as 0.3 microns in diameter, ULPA filters can remove 99.99% of the particulates that are 0.12 microns or more in diameter.
Knowing all this, you can see there is still risk of insufflated intraabdominal CO2 to leak into the OR’s room air (from port site air leaks, valves getting stuck in the open position, ports sliding out, during instrument exchanges, during specimen extraction, etc).
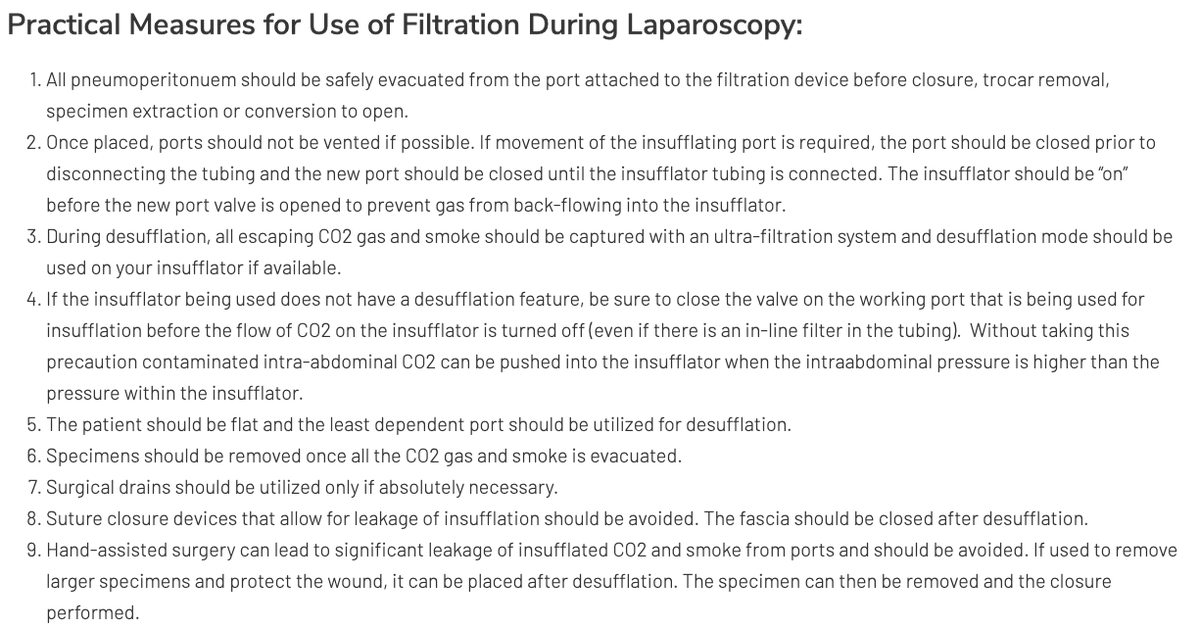
For this reason, societies have published strategies to prevent/minimize this from happening (see pic, SAGES sages.org/resources-smok…)
As for dealing with the next problem in filtration of potential aerosolized virus that escapes the operative field, we turn our attention to masks. Lots has been written and recommended on appropriate use of PPE and N95 masks.
"N95 respirators made by different companies were found to have different filtration efficiencies for the most penetrating particle size (0.1 to 0.3 micron), but all were at least 95% efficient at that size for NaCl particles” (ncbi.nlm.nih.gov/pubmed/9487666).
To obtain the stated filtration rate, N95 masks require a fit test and a tight seal around the mouth and nose to afford maximal (yet still imperfect) benefit. Surgical masks on the other hand are loose fitting simple disposable barriers and offer little in the way of filtration.

