
Just scoped a patients with GI bleed 🩸 BUT no pathology identified❓
Following the @ScopingSundays GI bleed theme and inspired by @ebtapper let me try and share some practical tips / thought process as a #tweetorial #GItwitter #MedTwitter
1/
Following the @ScopingSundays GI bleed theme and inspired by @ebtapper let me try and share some practical tips / thought process as a #tweetorial #GItwitter #MedTwitter
1/
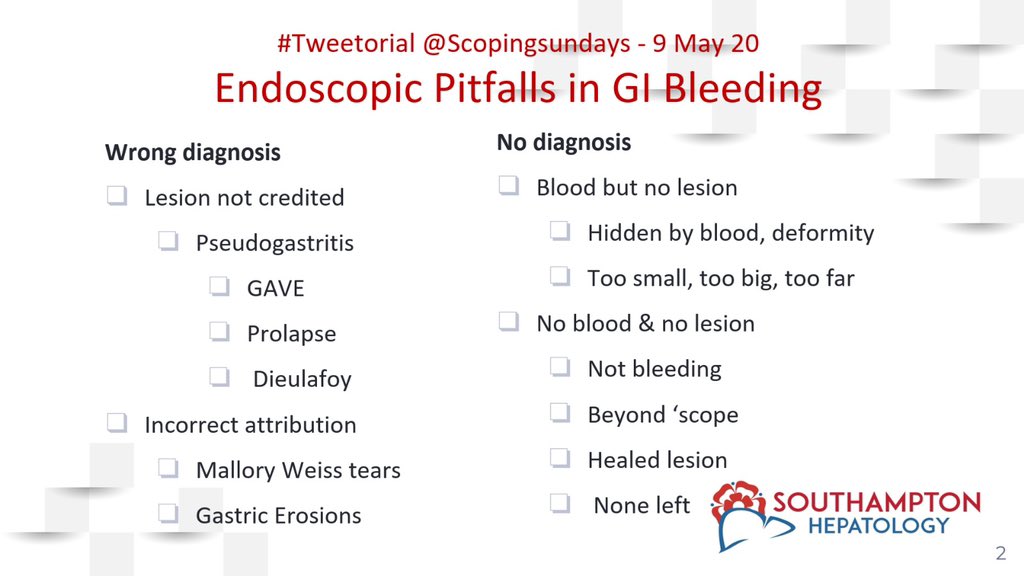
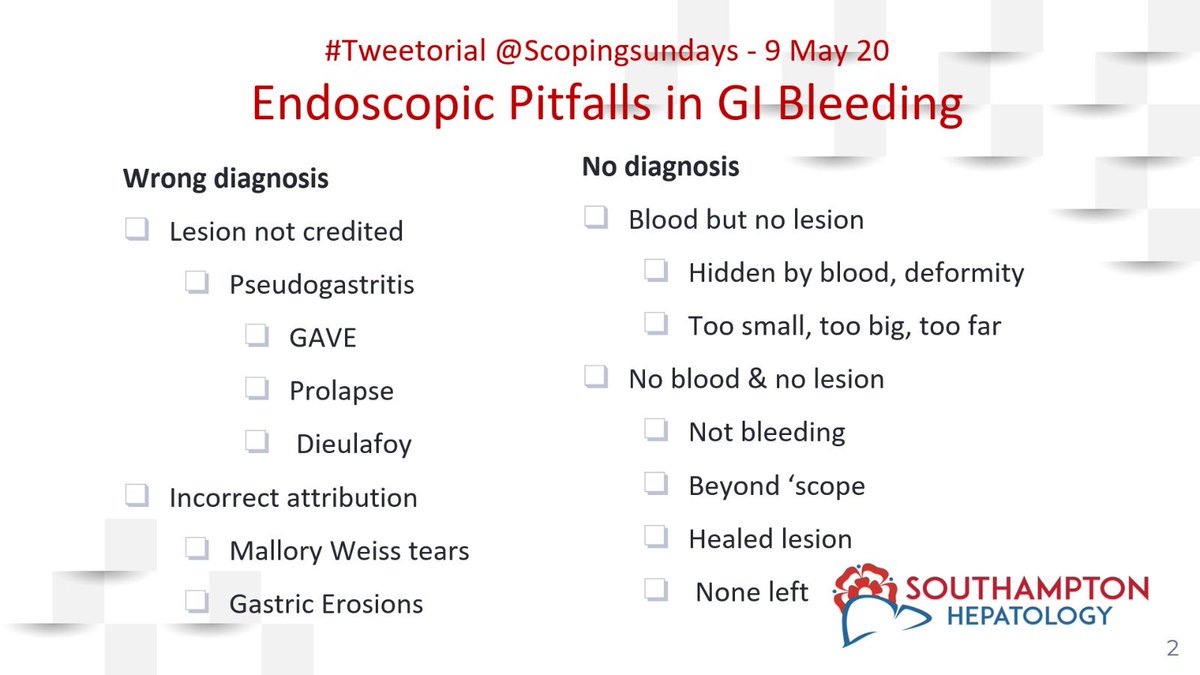
GI bleed 🩸- ‘Normal endoscopy’
▶️ No endoscopic Dx
(10% no source established)
Dagradi et al. Am.J.Gastroent
Or
▶️ Wrong endoscopic Dx
2/
▶️ No endoscopic Dx
(10% no source established)
Dagradi et al. Am.J.Gastroent
Or
▶️ Wrong endoscopic Dx
2/
No Endoscopix Dx
➕ Blood 🩸 but NO lesion
➖ No blood 🩸 & NO lesion
3/
➕ Blood 🩸 but NO lesion
➖ No blood 🩸 & NO lesion
3/
No endoscopic Dx
⬇️
Blood 🩸 BUT no lesion
⬇️
Obscured by blood - suck, 🧼 wash, clean, roll or elevate the head end as @dr_zaidi @JacquelineChuMD
had earlier suggested
4/
⬇️
Blood 🩸 BUT no lesion
⬇️
Obscured by blood - suck, 🧼 wash, clean, roll or elevate the head end as @dr_zaidi @JacquelineChuMD
had earlier suggested
4/
Uncleared Fundal Blood Pool
▪️12% Bleeders blood pool can’t be cleared
(51% Varices. 20% Gastric ulcer)
▪️More morbidity & Greater mortality
(Length of stay, blood transfusion, rebleeding)
Stollman et al. Gastrointest.Endosc.
5/
▪️12% Bleeders blood pool can’t be cleared
(51% Varices. 20% Gastric ulcer)
▪️More morbidity & Greater mortality
(Length of stay, blood transfusion, rebleeding)
Stollman et al. Gastrointest.Endosc.
5/
Going back to ...
No endoscopic Dx
⬇️
Blood 🩸 BUT no lesion
⬇️
Consider ‘small lesion with big potential’ i.e. Dieulafoy lesion
6/
No endoscopic Dx
⬇️
Blood 🩸 BUT no lesion
⬇️
Consider ‘small lesion with big potential’ i.e. Dieulafoy lesion
6/
Paul Georges (1839-1911)was French Physician & Surgeon - Classic description of appendicitis & Dieulafoy lesion (source - #Wikipedia)
7/
7/

Dieulafoy lesion:
▪️Recurrent often massive bleeds
▪️Large submucosal artery
(80% within 6 cm of GOJ)
▪️Bleed from superficial erosion, infiltration & rupture
▪️Control with adrenaline then clip/ablate (avoid haemopray)
8/
▪️Recurrent often massive bleeds
▪️Large submucosal artery
(80% within 6 cm of GOJ)
▪️Bleed from superficial erosion, infiltration & rupture
▪️Control with adrenaline then clip/ablate (avoid haemopray)
8/

Recap:
No endoscopic Dx
⬇️
Blood but no lesion
⬇️
Suck/wash/clean/roll/elevate the head end
⬇️
If it’s not a dieulafoy lesion
⬇️
Don’t forget the lesion which VANISHES with Anaemia
🔻🔻🔻
Focal MVA
9/
No endoscopic Dx
⬇️
Blood but no lesion
⬇️
Suck/wash/clean/roll/elevate the head end
⬇️
If it’s not a dieulafoy lesion
⬇️
Don’t forget the lesion which VANISHES with Anaemia
🔻🔻🔻
Focal MVA
9/
Focal Mucosal Vascular Anomaly
🔸 Less apparent when anaemic
🔸 present with anaemia & minor bleeds
🔸 Anywhere in the gut (Mucosal / submucosal)
🔸 Asso with
- skin telangiectasiae
- blue rubber bleb nevus synd
- coagulopathies
- aortic VD or not ‘Heyde’s syndrome’?
10/
🔸 Less apparent when anaemic
🔸 present with anaemia & minor bleeds
🔸 Anywhere in the gut (Mucosal / submucosal)
🔸 Asso with
- skin telangiectasiae
- blue rubber bleb nevus synd
- coagulopathies
- aortic VD or not ‘Heyde’s syndrome’?
10/
No endoscopic Dx
⬇️
Blood but no lesion
⬇️
Suck/wash/clean/roll/elevate the head end
⬇️
If it’s not a dieulafoy lesion
⬇️
If Its not a Focal MVA
⬇️
Lesion beyond reach of the scope⁉️
What comes to your mind❓
11/
⬇️
Blood but no lesion
⬇️
Suck/wash/clean/roll/elevate the head end
⬇️
If it’s not a dieulafoy lesion
⬇️
If Its not a Focal MVA
⬇️
Lesion beyond reach of the scope⁉️
What comes to your mind❓
11/
We owe this gent a lot of lives‼️
Johann Friedrich Meckel 1781 – 1833
German anatomist and embryologist who described the vestigial omphalomesenteric duct
Present in 2% of population
12/
Johann Friedrich Meckel 1781 – 1833
German anatomist and embryologist who described the vestigial omphalomesenteric duct
Present in 2% of population
12/
Lesions beyond reach of scope
🔹 Meckel’s diverticulum
🔹 Ulcerative jejunitis (h/o Coeliac dis❓)
🔹 Aorto-enteric fistula - EXSANGUINATE - Think CT‼️
🔹 Haemobilia - Numerous causes - Bleed then jaundice (ERCP vs IR)
13/
🔹 Meckel’s diverticulum
🔹 Ulcerative jejunitis (h/o Coeliac dis❓)
🔹 Aorto-enteric fistula - EXSANGUINATE - Think CT‼️
🔹 Haemobilia - Numerous causes - Bleed then jaundice (ERCP vs IR)
13/
No endoscopic Dx
⬇️
🩸 but no lesion
⬇️
⛔️ dieulafoy lesion
⛔️ Focal MVA
⛔️Lesion beyond reach of the scope
⬇️
❓ hidden in deformity
🔻Look for pyloric canal / asymmetry
🔻Duodenal (oedema / flask ulcers)
🔻Stomal ‼️ retriever in jejunum‼️
14/
⬇️
🩸 but no lesion
⬇️
⛔️ dieulafoy lesion
⛔️ Focal MVA
⛔️Lesion beyond reach of the scope
⬇️
❓ hidden in deformity
🔻Look for pyloric canal / asymmetry
🔻Duodenal (oedema / flask ulcers)
🔻Stomal ‼️ retriever in jejunum‼️
14/
Let’s SHIFT the focus like my patient
No Endoscopic diagnosis
⬇️
No blood
⬇️
❓Not actually bleeding – anaemic on iron + diarrhoea
❓Not UGIB – Burgundy stool
❓Healed lesion
Rarely: sudden massive bleed with none left
Or as we discussed Bleeding beyond reach❓
15/
No Endoscopic diagnosis
⬇️
No blood
⬇️
❓Not actually bleeding – anaemic on iron + diarrhoea
❓Not UGIB – Burgundy stool
❓Healed lesion
Rarely: sudden massive bleed with none left
Or as we discussed Bleeding beyond reach❓
15/
▶️ ‘Lesions are seen but not believed to be cause’
e.g.
♦️GAVE & Prolapse Gastropathy reported as Gastritis‼️
♦️Dieulafoy lesion reported as small gastric erosions ‼️
16/
e.g.
♦️GAVE & Prolapse Gastropathy reported as Gastritis‼️
♦️Dieulafoy lesion reported as small gastric erosions ‼️
16/
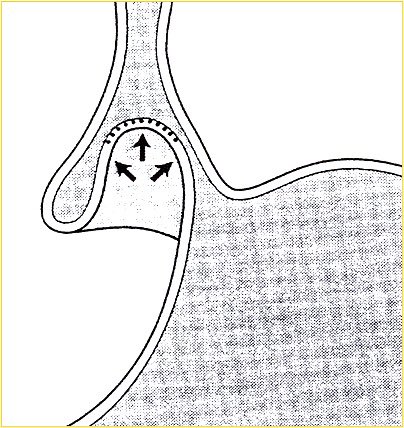
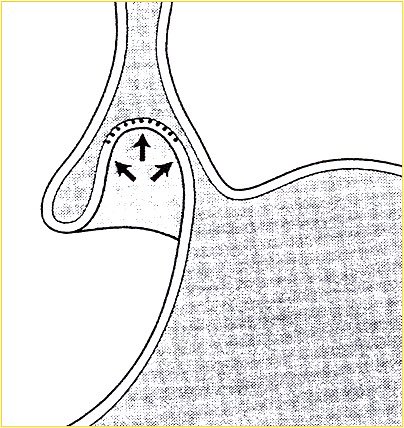
Prolapse Gastropathy is not as innocent as it may seem & can present with haematemesis❗️
🔹Caused by retching
🔹Described by Tony Axon (ex Pres. BSG) @BritSocGastro
🔹Leaves sharply demarcated area of erythema/oozing
🔹Looks like focal gastritis
17/
🔹Caused by retching
🔹Described by Tony Axon (ex Pres. BSG) @BritSocGastro
🔹Leaves sharply demarcated area of erythema/oozing
🔹Looks like focal gastritis
17/
Lesion appears to be cause but is not ⁉️
♦️ Mallory Weiss tear
‘Tear is often a marker of another significant bleeding source’
MacCulloch S & Rose JDR 1999
18/
♦️ Mallory Weiss tear
‘Tear is often a marker of another significant bleeding source’
MacCulloch S & Rose JDR 1999
18/

So how to deal with MW tear❓
▪️Not bleeding
▪️No “visible vessel”
▪️Mild bleed
⬇️
No treatment
▪️Big bleed
▪️“visible vessel”
▪️Continued bleeding
⬇️
Injection or mechanical
19/
▪️Not bleeding
▪️No “visible vessel”
▪️Mild bleed
⬇️
No treatment
▪️Big bleed
▪️“visible vessel”
▪️Continued bleeding
⬇️
Injection or mechanical
19/
▶️ ‘Lesions are seen but not believed to be cause’
e.g.
♦️GAVE & Prolapse Gastropathy reported as Gastritis‼️
♦️Dieulafoy lesion reported as small gastric erosions ‼️
16/
e.g.
♦️GAVE & Prolapse Gastropathy reported as Gastritis‼️
♦️Dieulafoy lesion reported as small gastric erosions ‼️
16/
Prolapse Gastropathy is not as innocent as it may seem & can present with haematemesis❗️
🔹Caused by retching
🔹Described by Tony Axon (ex Pres. BSG) @BritSocGastro
🔹Leaves sharply demarcated area of erythema/oozing
🔹Looks like focal gastritis
17/
🔹Caused by retching
🔹Described by Tony Axon (ex Pres. BSG) @BritSocGastro
🔹Leaves sharply demarcated area of erythema/oozing
🔹Looks like focal gastritis
17/
Lesion appears to be cause but is not ⁉️
♦️ Mallory Weiss tear
‘Tear is often a marker of another significant bleeding source’
MacCulloch S & Rose JDR 1999
18/
♦️ Mallory Weiss tear
‘Tear is often a marker of another significant bleeding source’
MacCulloch S & Rose JDR 1999
18/

So how to deal with MW tear❓
▪️Not bleeding
▪️No “visible vessel”
▪️Mild bleed
⬇️
No treatment
▪️Big bleed
▪️“visible vessel”
▪️Continued bleeding
⬇️
Injection or mechanical
19/
▪️Not bleeding
▪️No “visible vessel”
▪️Mild bleed
⬇️
No treatment
▪️Big bleed
▪️“visible vessel”
▪️Continued bleeding
⬇️
Injection or mechanical
19/
@threadreaderapp unroll please

