🚨Crashing Patient Case🚨
72 yo ♀️ to ED with syncope, hypotension. Intubated for hypercap/hypox resp failure. Hypotensive post, tx to ICU.
A Tubed
B FiO2 1.0, 10 ml/kg Vt
❤️ MAP 70 -> 50 -> 30 in mins
D sedate, +cough
E Leaky 22g PIV
U n/a
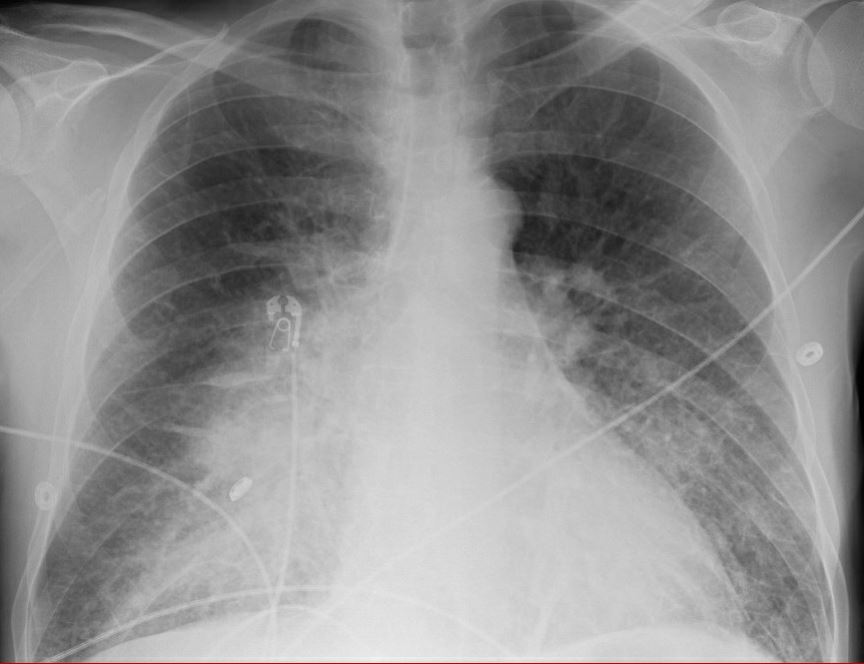
L WBC 35k, lact 1.7, UA+CXR shown
72 yo ♀️ to ED with syncope, hypotension. Intubated for hypercap/hypox resp failure. Hypotensive post, tx to ICU.
A Tubed
B FiO2 1.0, 10 ml/kg Vt
❤️ MAP 70 -> 50 -> 30 in mins
D sedate, +cough
E Leaky 22g PIV
U n/a
L WBC 35k, lact 1.7, UA+CXR shown


First step?
My team is very adept at CVCs, but we go for the IO (1 min to insert vs 10, and much higher first past success doi.org/10.1097/ccm.00…)
More on IOs from LITFL litfl.com/intraosseous-a…
Also, the vent is alarming for high peak pressures (45 cm H2O consistently). What next?
More on IOs from LITFL litfl.com/intraosseous-a…
Also, the vent is alarming for high peak pressures (45 cm H2O consistently). What next?
Norepi is started via IO and rapidly escalating (0.1 -> 1 mcg/kg/min in minutes).
Disconnecting vent is reasonable, but not diagnostic.
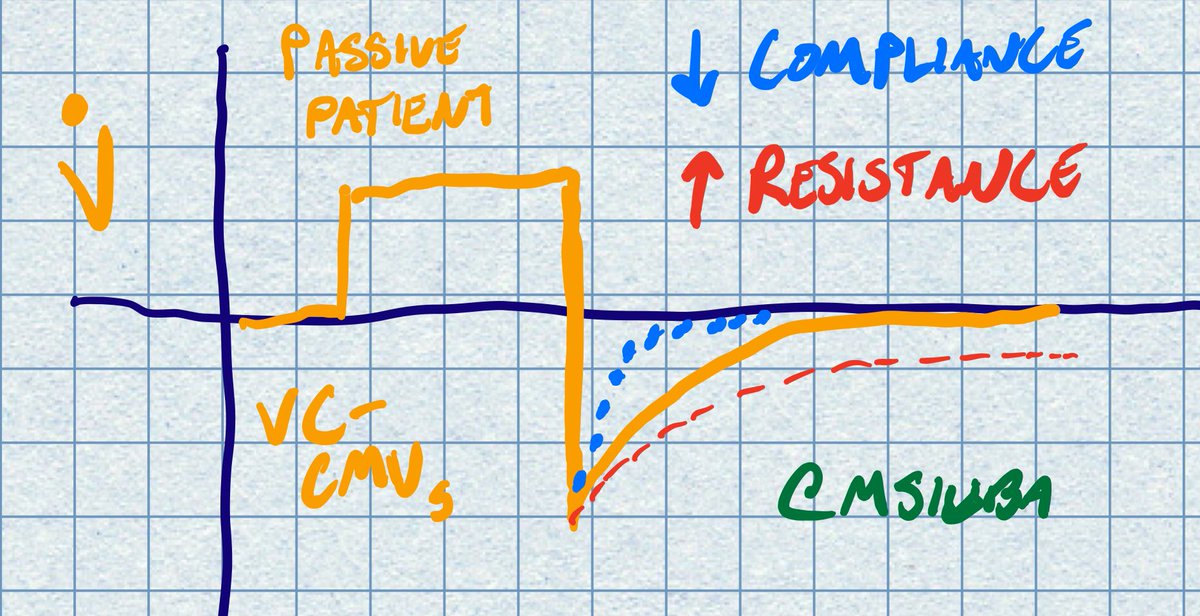
Plateau pressure is 42. What is *not* a possible explanation?
Disconnecting vent is reasonable, but not diagnostic.
Plateau pressure is 42. What is *not* a possible explanation?
This is clearly a compliance problem. More on airway pressures here: litfl.com/high-airway-an…
Your colleague is grabbing the POCUS machine. The *first* thing you do now is lower the tidal volume to 6 ml/kg. Airway pressures now Ppeak 34 and Pplat 31 on PEEP 8.
Your colleague is grabbing the POCUS machine. The *first* thing you do now is lower the tidal volume to 6 ml/kg. Airway pressures now Ppeak 34 and Pplat 31 on PEEP 8.
Simply by virtue of dropping the tidal volume, pressor dose is decreased by *half* (now 0.5 mcg/kg/min norepi).
Notable RUSH Exam Findings (sorry for paucity of images given emergency):
Echo: no effusion, normal LV/RV size and fxn. Midrange IVC with respirophasic variation
Notable RUSH Exam Findings (sorry for paucity of images given emergency):
Echo: no effusion, normal LV/RV size and fxn. Midrange IVC with respirophasic variation
Lung exam:
L: A lines throughout with +lung slide
R: Apical A lines, mid B lines, basilar consolidation with this septated effusion
RUSH otherwise neg. More on exam here: emcrit.org/rush-exam/orig…
L: A lines throughout with +lung slide
R: Apical A lines, mid B lines, basilar consolidation with this septated effusion
RUSH otherwise neg. More on exam here: emcrit.org/rush-exam/orig…

To drain, or not to drain? UA was positive. Also PMH notabel for lung cancer receiving chemorad.
Case resolution to follow tomorrow!
Case resolution to follow tomorrow!
Let's continue!
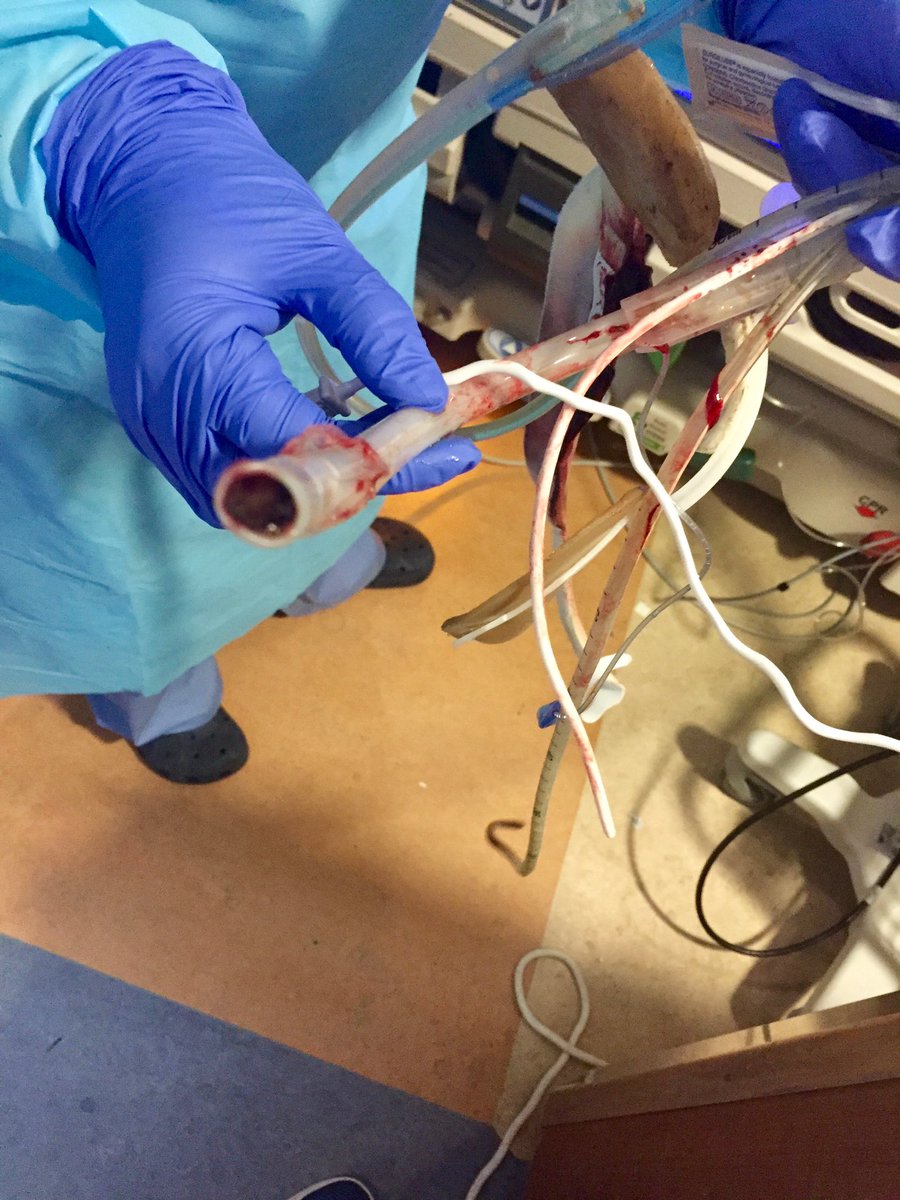
Given degree of shock and unclear etiology, we drained it.
The US had some features of complex effusion (esp septations), though hx of malignancy made the nature of the effusion less clear pre-tap. Because of the complexity, pigtail cath was used. Guidewire here
Given degree of shock and unclear etiology, we drained it.
The US had some features of complex effusion (esp septations), though hx of malignancy made the nature of the effusion less clear pre-tap. Because of the complexity, pigtail cath was used. Guidewire here

Initial drainage was cloudly yellow, but mostly translucent.
Studies shown here.
Studies shown here.

What's the likely diagnosis?
Initial gram stain positive for GPCs, eventually grows pneumococcus (also 2/2 blood cultures positive).
Effusion was situated anterior-laterally, with septations. Any other interventions you'd take?
Effusion was situated anterior-laterally, with septations. Any other interventions you'd take?
Given the location, highly concerning for loculated effusion.
TPA/DNAse was instilled. One hour later, additional 100 ml of frank purulent drainage was obtained.
Over the next 24 hours, pressors weaned off. 24 hours after that, the patient is extubated, quickly move out of ICU
TPA/DNAse was instilled. One hour later, additional 100 ml of frank purulent drainage was obtained.
Over the next 24 hours, pressors weaned off. 24 hours after that, the patient is extubated, quickly move out of ICU
Pneumococcal empyema is not a rare entity. Why share this case?
#GoldenHour mentality (cc @ogi_gajic): We placed IO, tweaked the vent, gave antibiotics & hydrocortisone in the first hour in ICU.
#GoldenHour mentality (cc @ogi_gajic): We placed IO, tweaked the vent, gave antibiotics & hydrocortisone in the first hour in ICU.
It's easy to think of a #zentensivist as hands off.
However, we aim to apply *just* the right amount of intervention to right the ship. This is required (esp in terms of ABCs, time to abx, source control) in order to prevent further harm and needed interventions
However, we aim to apply *just* the right amount of intervention to right the ship. This is required (esp in terms of ABCs, time to abx, source control) in order to prevent further harm and needed interventions
This patient left ICU without acquiring any added organ failures despite the initial severity of illness. I certainly can't prove it was our behavior. However, this speaks to timely intervention on behalf of our team (RN, RT, APP, etc).
It would have been easy to blame the effusion on malignancy (we had no prior imaging), and the patient could have suffered for premature closure.
Thanks for playing along!
What else did you learn or think of in this case? /end
Thanks for playing along!
What else did you learn or think of in this case? /end