
Feels so good to be back to #Neurology. Today I had the pleasure to give #Neurologymorningreport on Necrotizing Autoimmune Myopathy #NAM. #MedTwitter follow below a few pearls I shared with the team @ErsidaBuraniqi @nzalewski2. THREAD. 
#NAM is an autoimmune myopathy characterized by severe proximal weakness, myofiber necrosis with minimal or no inflammatory infiltrates on muscle biopsy, and infrequent extra-muscular involvement.
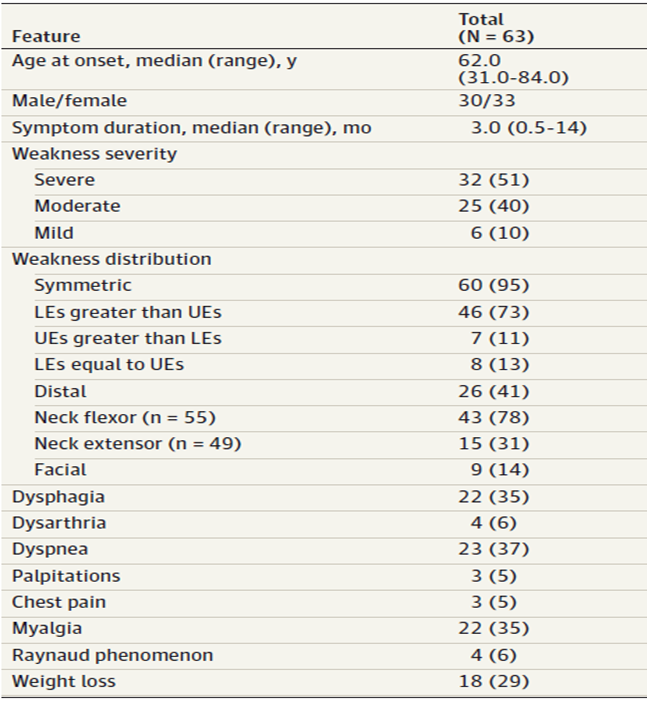
- Usually presents with subacute/chronic severe proximal weakness. Neck weakness is common and dysphagia occurs in aproximately 1/3
- EMG shows proximal myopathy with fibrillation potentials
- CK is usually markedly elevated (in the thousands range)
ja.ma/3g9FWaz
- EMG shows proximal myopathy with fibrillation potentials
- CK is usually markedly elevated (in the thousands range)
ja.ma/3g9FWaz
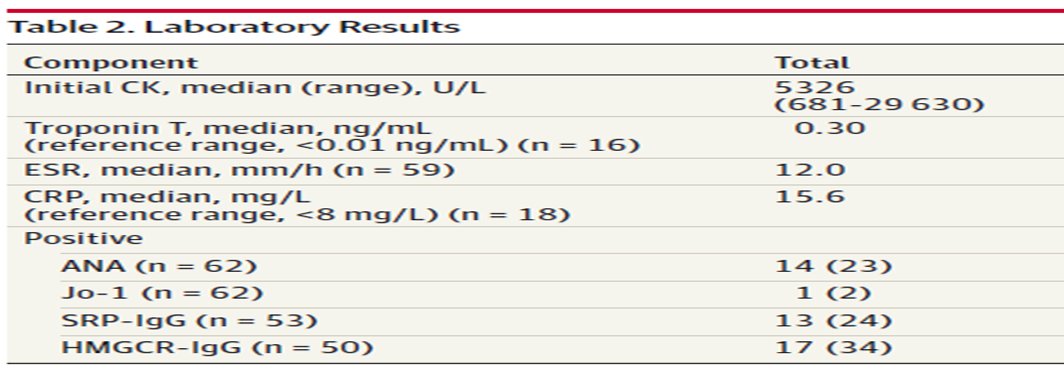
- 1/3 Anti-HMGCR ab positive, 1/3 Anti-SRP ab positive and 1/3 seronegative NAM
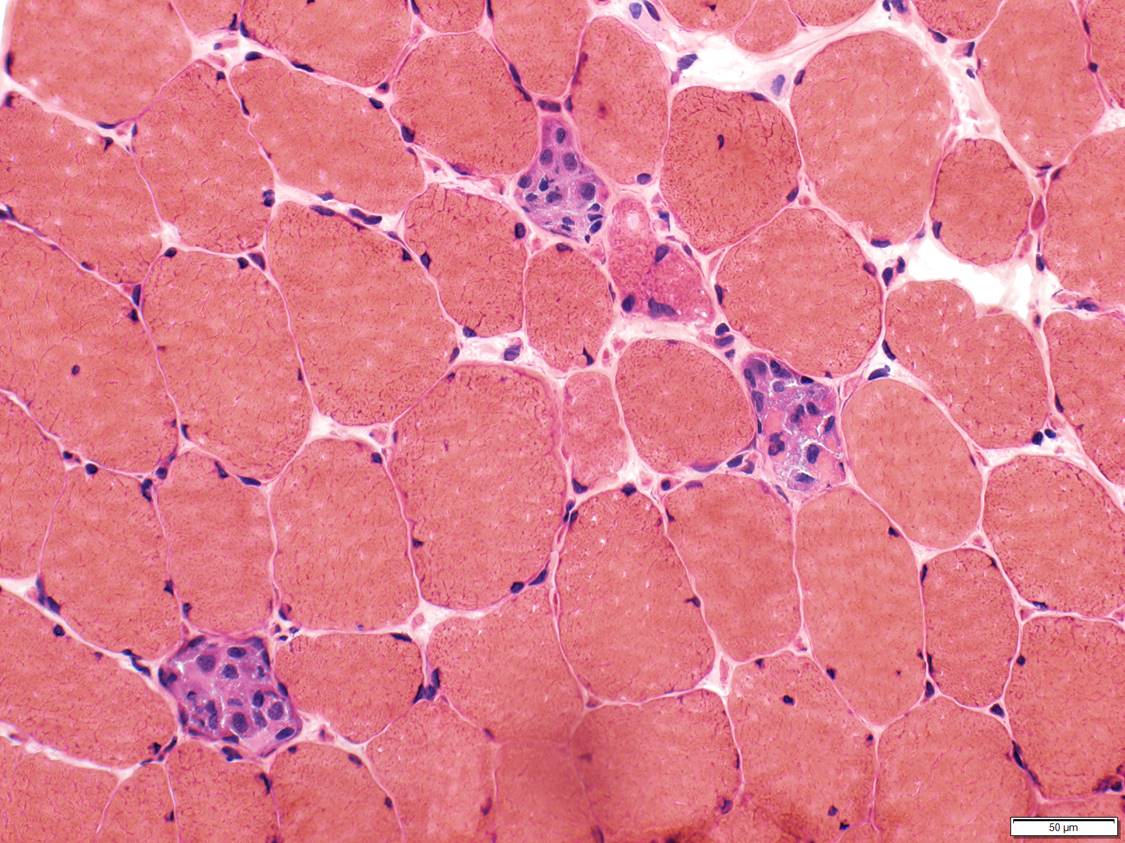
-Muscle biopsy usually shows scattered necrotic or regenerating fibers, and no or minimal inflammation. Supports the diagnosis, but more important for differential diagnosis rdcu.be/b4iFC
-Muscle biopsy usually shows scattered necrotic or regenerating fibers, and no or minimal inflammation. Supports the diagnosis, but more important for differential diagnosis rdcu.be/b4iFC
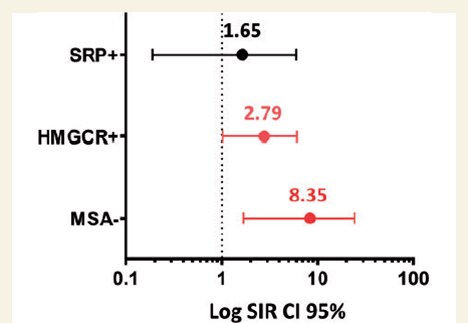
- High risk of cancer – especially in seronegative NAM and anti-HMGCR +
- Cancer screening in all NAM patients regardless of ab status
- Strongly consider whole body PET CT plus appropriate cancer screening by age
academic.oup.com/brain/article/…
- Cancer screening in all NAM patients regardless of ab status
- Strongly consider whole body PET CT plus appropriate cancer screening by age
academic.oup.com/brain/article/…
Main differential diagnosis
- Other auto-immune myopathies (dermatomyositis, anti-synthetase sd or overlap myositis)
- Sporadic Late onset nemaline myopathy
- Amyloid myopathy
- Sarcoid myopathy
- Other auto-immune myopathies (dermatomyositis, anti-synthetase sd or overlap myositis)
- Sporadic Late onset nemaline myopathy
- Amyloid myopathy
- Sarcoid myopathy
Work up
- CBC, CMP, TSH, CK and HIV
- Connective tissue cascade and ENAs
- Myomarker 3 panel
- Anti-HMGCR and Anti-SRP abs (necrotizing myopathy panel)
- Monoclonal gammopathy screen (SPEP, IF and free light chains)
- Cancer screening, ideally whole body PET-CT
- Muscle biopsy
- CBC, CMP, TSH, CK and HIV
- Connective tissue cascade and ENAs
- Myomarker 3 panel
- Anti-HMGCR and Anti-SRP abs (necrotizing myopathy panel)
- Monoclonal gammopathy screen (SPEP, IF and free light chains)
- Cancer screening, ideally whole body PET-CT
- Muscle biopsy
Treatment
- We usually combine IV solumedrol with IVIg for at least 4 months, and then see patient back.
- If patient does not have cancer, we start a steroid-sparing agent (AZA, MTX or CellCelpt) in the beginning of the trial
- We usually combine IV solumedrol with IVIg for at least 4 months, and then see patient back.
- If patient does not have cancer, we start a steroid-sparing agent (AZA, MTX or CellCelpt) in the beginning of the trial
- In the Mayo series, dual immunotherapy had an odds ratio for significantly improvement/return to baseline of 15.6
- Anti-SRP +: more severe, may respond best to regimens that include rituximab
- Anti-HMGCR +: IVIg may be the most effective
- Seronegative: worst prognosis
- Anti-SRP +: more severe, may respond best to regimens that include rituximab
- Anti-HMGCR +: IVIg may be the most effective
- Seronegative: worst prognosis
- #NAM is treatable and treatment should be started early
- Consider Rituximab or Cytoxan in refractory cases, and referral to a tertiary neuromuscular center
- Consider Rituximab or Cytoxan in refractory cases, and referral to a tertiary neuromuscular center

