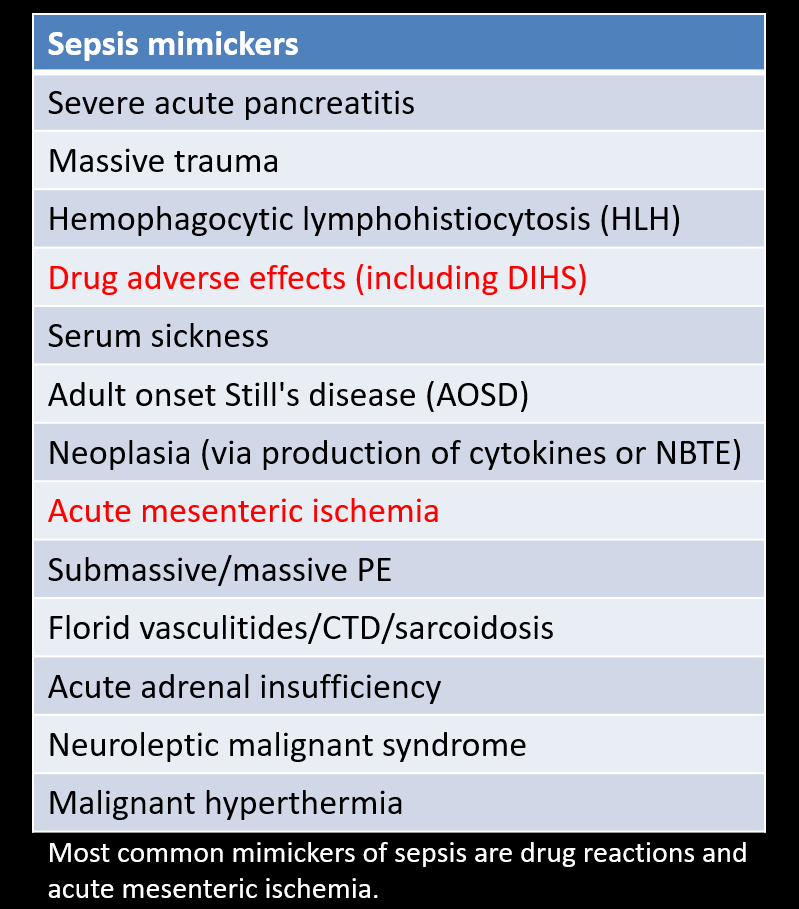
1/ My patient has tachycardia, fevers and lactic acidosis. Does he/she have sepsis? Heffner et. al found that, up to 18% of patients with SIRS, initially diagnosed as sepsis, had a non-septic SIRS also known as "sepsis mimicker". #Tweetorial
2/ A 30-ish y.o. patient with history of type 1 diabetes mellitus, essential hypertension & asthma presented to the ED with a 2-day history of dry cough. No dyspnea, chest pain, documented fevers, sweats, rhinorrhea or sore throat. Mentions 30-lb wt loss + fatigue last 6 months.
3/ Patient stopped working due to fatigue. Diabetes is well controlled (A1c 7.5%). Patient smokes cigarettes, drinks socially and denies using drugs. No vaping.
On presentation: BP 150/110, HR 134, RR 20, SpO2 98%, Tm 99.5F.
On presentation: BP 150/110, HR 134, RR 20, SpO2 98%, Tm 99.5F.
4/ Few initial thoughts:
- Cough is acute (foreground). Wt loss + fatigue are chronic (background).
- Is cough the culmination of a chronic disease or a superimposed phenomenon?
- Wt loss + decent oral intake suggests calorie expenditure > calorie intake a.k.a. hypermetabolism.
- Cough is acute (foreground). Wt loss + fatigue are chronic (background).
- Is cough the culmination of a chronic disease or a superimposed phenomenon?
- Wt loss + decent oral intake suggests calorie expenditure > calorie intake a.k.a. hypermetabolism.
5/ Quick exam: thin-appearing, does not look sick, tachycardic/regular, CTAB, tender in RUQ of abdomen, no skin rash.
6/ Initial labs: WBC 8.2, Hgb 13.3, Plts 348, BMP unremarkable, albumin 3.7, protein 9.6, ALP 312, AST 65, ALT 49, bili 0.3, INR 1.2, Ca 10.4, ketones normal, lactic acid 2.9-->3.3-->4.8, ESR 126, CRP 4.3, HIV-, TSH 1.9, UA w/ 2+ protein. Highlights?
7/ CXR to the left, compared to old one from 2017. Seems overall more hazy. Poorly penetrated by x-rays? No clear alveolar infiltrates. Hilar prominence? 

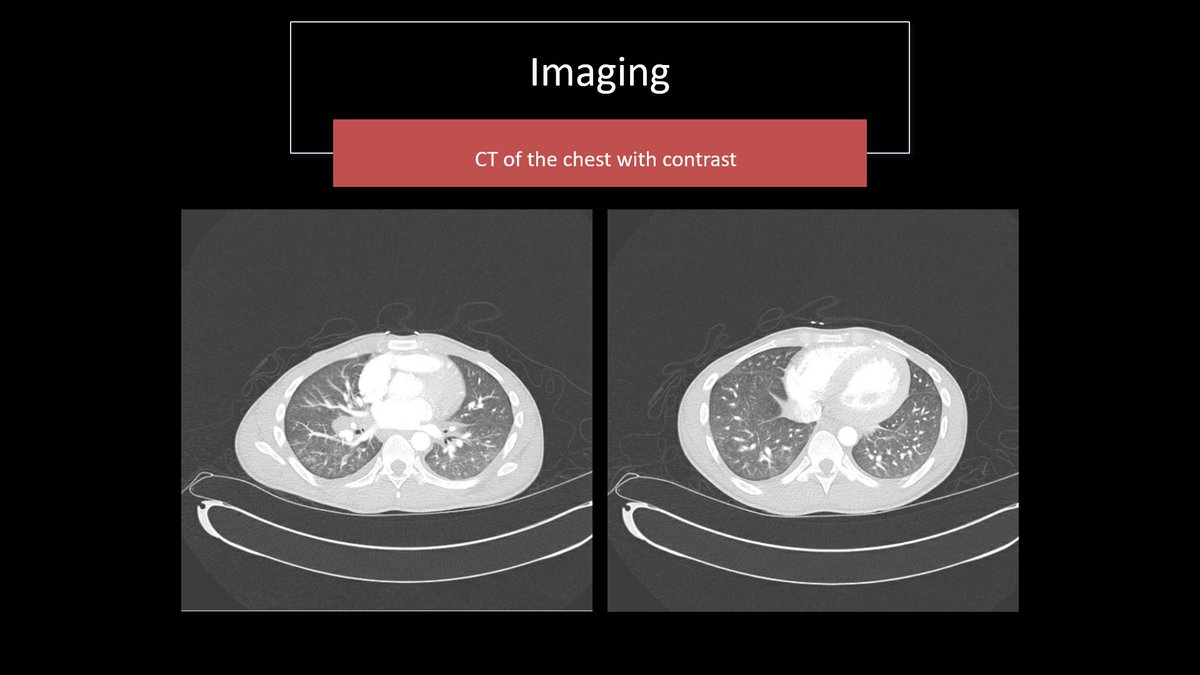
8/ Haziness is real indeed. CT shows tree-in-bud and faint ground glass opacities. Mention of reactive hilar and mediastinal lymphadenopathies. Is this septic pneumonia? But how to explain chronic weight loss?🤔
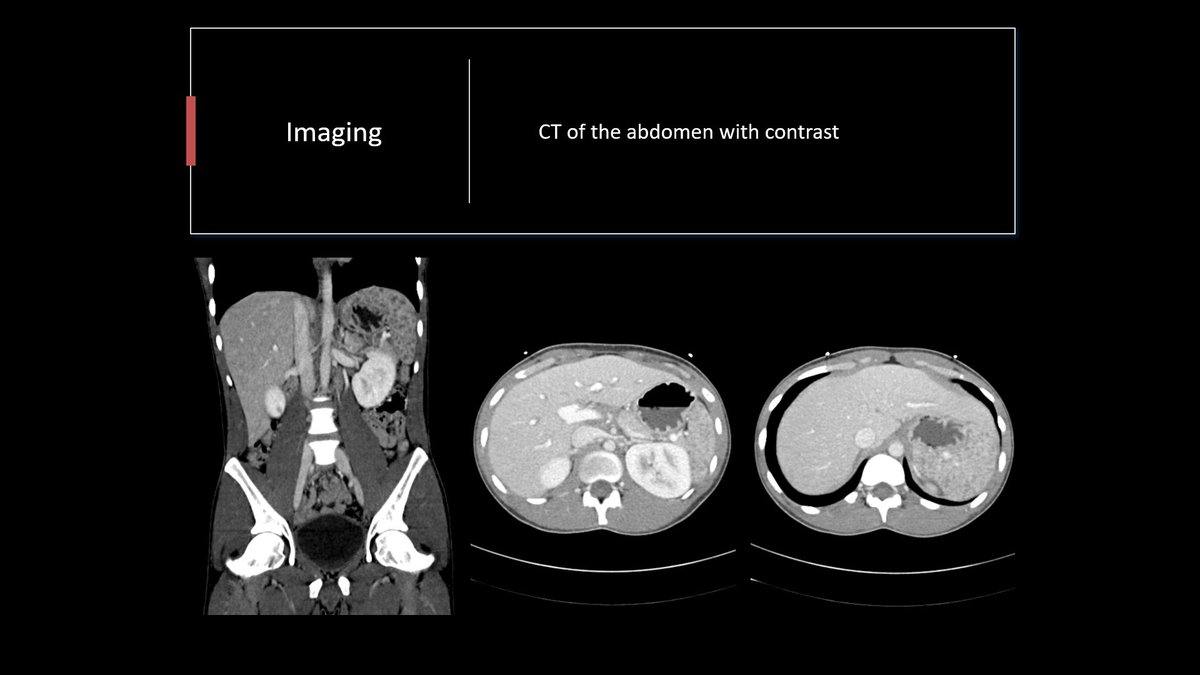
9/ The plot thickens. CT of the abdomen reveals hepatosplenomegaly. Spleen and liver full of innumerable hypoenhancing nodules. This is what @MedEdPGH would call the "rabbit hole". Chase the most esoteric finding in presentation.
10/ Time for a quick PR:
30-ish y.o. with history of T1DM and HTN presenting with acute dry cough and a background of wt loss & fatigue. Found to have tachycardia, inflammation, lactic acidosis and cholestatic liver injury. CT with hepatosplenomegaly and small hypodense lesions.
30-ish y.o. with history of T1DM and HTN presenting with acute dry cough and a background of wt loss & fatigue. Found to have tachycardia, inflammation, lactic acidosis and cholestatic liver injury. CT with hepatosplenomegaly and small hypodense lesions.
11/ Given patient’s significant tachycardia, ⬆️inflammatory markers and lactic acidosis, a tentative no-miss diagnosis of sepsis was made in the ED.
Patient was treated with 4L of IV fluids and was started on broad spectrum antibiotics.
Patient was treated with 4L of IV fluids and was started on broad spectrum antibiotics.
11(cont'd)/ He was never febrile. He did not look sick. He did not have a significant leukocytosis or leukopenia.
Despite this treatment, patient’s tachycardia persisted and his HR was up to mid-120s twelve hours later.
Not your typical sepsis illness script, eh?
Despite this treatment, patient’s tachycardia persisted and his HR was up to mid-120s twelve hours later.
Not your typical sepsis illness script, eh?
12/ Now that antibiotics are in, we can sit down and try to interpret these lung, liver & spleen lesions.
Differentials include lymphoma, TB, atypical mycobacteriosis, endemic mycoses, sarcoidosis, amyloidosis. If immunosuppressed, can add nocardiosis, aspergillosis, cryptococcus
Differentials include lymphoma, TB, atypical mycobacteriosis, endemic mycoses, sarcoidosis, amyloidosis. If immunosuppressed, can add nocardiosis, aspergillosis, cryptococcus
13/ More labs: Blasto Ag, Histo Ag/Ab, Crypto Ag, IGRA all negative. Respiratory viral panel negative. COVID-19 negative. Monospot negative. Sputum culture growing scan amounts of S. agalactiae. ANA, ds-DNA, ANCAs negative. Can't diagnose with a serum biomarker? Sample tissue.
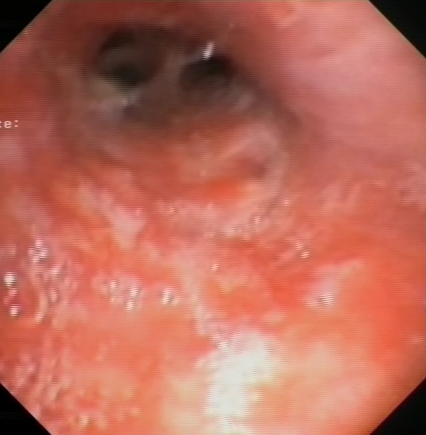
14/ A bronchoscopy was done and revealed:
- Cobblestoning of the mucosa, notably in RLL (see representative image).
- Enlarged subcarinal lymph node status post FNA.
- BAL RUL anterior segment, microbrushing and transbronchial biopsies RLL superior segment.
- Cobblestoning of the mucosa, notably in RLL (see representative image).
- Enlarged subcarinal lymph node status post FNA.
- BAL RUL anterior segment, microbrushing and transbronchial biopsies RLL superior segment.
15/ Path revealed:
Non-necrotizing granulomas.
AFB and GMS were negative.
No evidence of malignancy seen.
Non-necrotizing granulomas.
AFB and GMS were negative.
No evidence of malignancy seen.
16/ A diagnosis of disseminated sarcoidosis with multi-organ involvement mimicking severe sepsis was made.
Significant cholestatic liver injury attributed to liver infiltration. Lactic acidosis due to poor lactic acid clearance(?), cytokine-induced mitochondrial dysfunction(?).
Significant cholestatic liver injury attributed to liver infiltration. Lactic acidosis due to poor lactic acid clearance(?), cytokine-induced mitochondrial dysfunction(?).
17/ Patient was started on high dose steroids with rapid improvement in hemodynamics, clearance of lactic acid and ⬇️ in ALP.
Antibiotics were discontinued. No solid ground to call this syndrome "sepsis" was found.
Antibiotics were discontinued. No solid ground to call this syndrome "sepsis" was found.
18/ Teaching points:
- Non-septic SIRS or "sepsis mimickers" or "sterile inflammatory disorders" cause up to 20% of hospital SIRS presentations.
- While sepsis (SIRS + infection) is a no-miss diagnosis, one must entertain alternative diagnosis when things are not adding up.
- Non-septic SIRS or "sepsis mimickers" or "sterile inflammatory disorders" cause up to 20% of hospital SIRS presentations.
- While sepsis (SIRS + infection) is a no-miss diagnosis, one must entertain alternative diagnosis when things are not adding up.
18 (cont'd)/
Think of a non-septic SIRS when you have atypical features in presentation (Faget’s sign, lack of a source of infection & microbiological documentation within 24h, well-appearing and not feeling the fevers, lack of defervescence or change in hemodynamics despite AB
Think of a non-septic SIRS when you have atypical features in presentation (Faget’s sign, lack of a source of infection & microbiological documentation within 24h, well-appearing and not feeling the fevers, lack of defervescence or change in hemodynamics despite AB
19/ Some patients will still have late-confirmed sepsis (difficult-to-grow bugs, infection confirmed by serology).
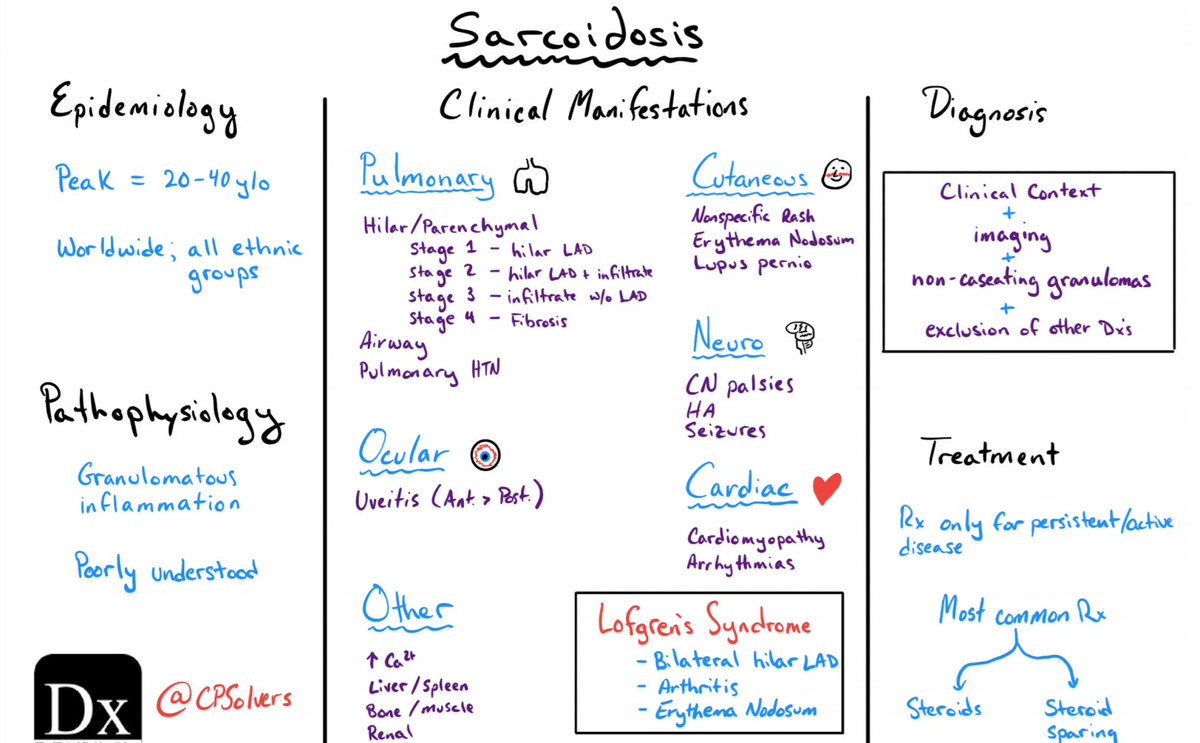
Thanks for tuning in. I leave you with a refresher schema from @CPSolvers on sarcoidosis:
Thanks for tuning in. I leave you with a refresher schema from @CPSolvers on sarcoidosis: