1/ There is more to serum protein electrophoresis (SPEP) than meets the eye. A SPEP is a rich exam, with a wealth of information, that has been relegated to the land of malignant hematology with advances in lab testing. Let's rediscover its richness through a few clinical cases. 
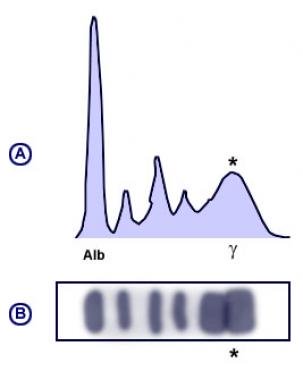
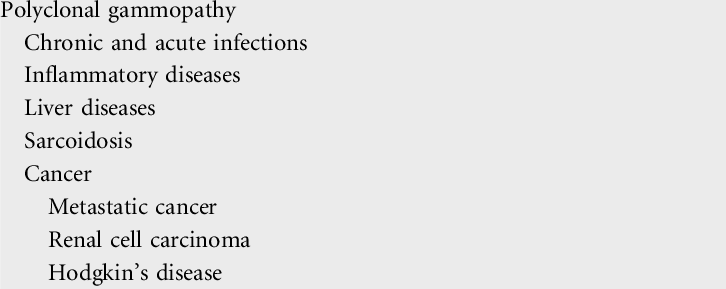
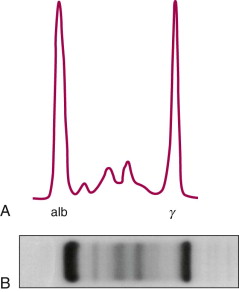
2/ This is what a normal SPEP pattern looks like. Albumin (60%) - globulins (40%). Normal A:G ratio 1.5-2.5.
Globulins comprise alpha 1, alpha 2, beta 1, beta 2 and gamma globulin portions.
Globulins comprise alpha 1, alpha 2, beta 1, beta 2 and gamma globulin portions.
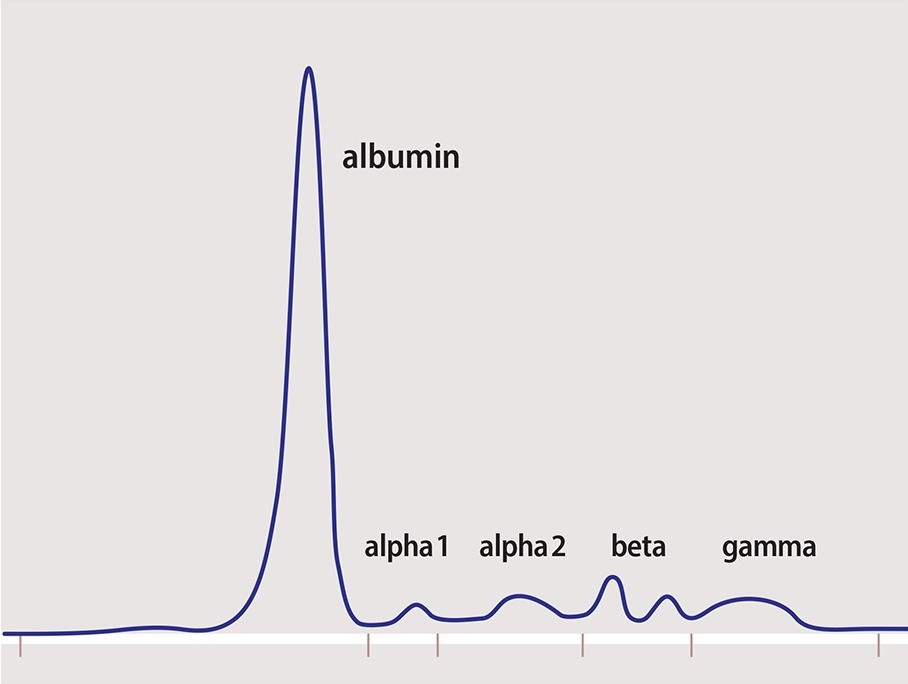
3/ Alpha 1 portion: contains alpha1-antitrypsin. Positive acute phase reactant. ⬇️in AAT deficiency, ⬆️in inflammation & pregnancy.
Alpha 2 portion: contains ceruloplasmin & haptoglobin. Positive acute phase reactant.
Alpha 2 portion: contains ceruloplasmin & haptoglobin. Positive acute phase reactant.
4/ Beta 1 portion: contains transferrin. Pre-β region contains VLDL.
Beta 2 portion: contains beta-lipoprotein (mainly LDL).
IgA and IgM are in beta portion of SPEP.
Iron deficiency anemia causes ⬆️ in transferrin and β1. Familial hypercholesterolemia causes a β2 spike.
Beta 2 portion: contains beta-lipoprotein (mainly LDL).
IgA and IgM are in beta portion of SPEP.
Iron deficiency anemia causes ⬆️ in transferrin and β1. Familial hypercholesterolemia causes a β2 spike.
5/ Gamma portion: main utility of SPEP.
If ⬇️, suspect humoral immune dysfunction w/ hypogammaglobulinemia.
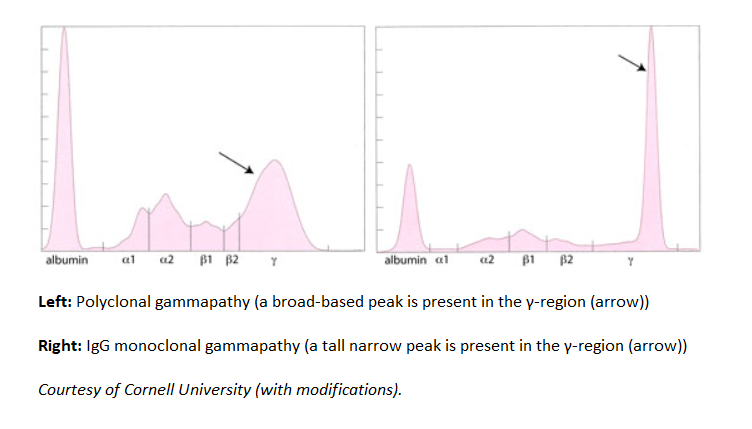
If ⬆️, suspect gammapathy and determine if monoclonal or polyclonal.
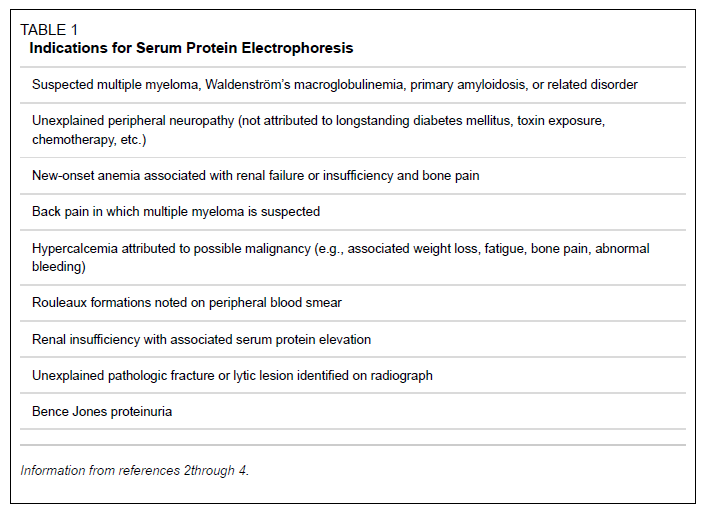
When to order a SPEP? (courtesy of AAFP, 2005)
If ⬇️, suspect humoral immune dysfunction w/ hypogammaglobulinemia.
If ⬆️, suspect gammapathy and determine if monoclonal or polyclonal.
When to order a SPEP? (courtesy of AAFP, 2005)
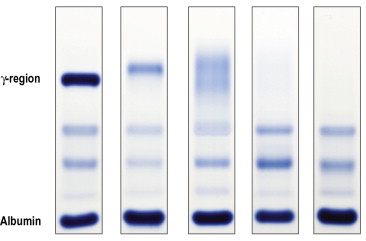
6/ Case #1:
What pathology is this pattern most compatible with?
What pathology is this pattern most compatible with?

6/ What pathology is this pattern most compatible with?
7/ Answer: Inflammation
Note ⬇️ albumin (➖acute phase reactant) & ⬆️α1/α2 (➕phase reactants).
Dehydration expected to cause ⬆️ albumin (hemoconcentration).
CVID expected to cause flattening of γ portion.
AAT def. causes flattening of α1 (SPEP now replaced w/ serum AAT level).
Note ⬇️ albumin (➖acute phase reactant) & ⬆️α1/α2 (➕phase reactants).
Dehydration expected to cause ⬆️ albumin (hemoconcentration).
CVID expected to cause flattening of γ portion.
AAT def. causes flattening of α1 (SPEP now replaced w/ serum AAT level).
8/ What pathology is this pattern most compatible with?
8/ What pathology is this pattern most compatible with?
9/ Answer: Nephrotic syndrome.
Loss of small-size proteins in urine (⬇️albumin, Ig) with compensatory ⬆️liver production of large proteins leading to α2 spike (α2-Macroglobulin & VLDL).
IDA can cause a β1 spike.
Loss of small-size proteins in urine (⬇️albumin, Ig) with compensatory ⬆️liver production of large proteins leading to α2 spike (α2-Macroglobulin & VLDL).
IDA can cause a β1 spike.
10/ Case #3:
What pathology is this pattern most compatible with?
What pathology is this pattern most compatible with?
10/ What pathology is this pattern most compatible with?
11/ Answer: cirrhosis
Early cirrhosis: beta-gamma bridging (related to increase in IgA and transferrin production?). Fairly characteristic of cirrhosis.
Advanced cirrhosis: poor synthetic function. ⬇️albumin.
A:G ratio<1 (⬇️albumin, ⬆️Ig).
Early cirrhosis: beta-gamma bridging (related to increase in IgA and transferrin production?). Fairly characteristic of cirrhosis.
Advanced cirrhosis: poor synthetic function. ⬇️albumin.
A:G ratio<1 (⬇️albumin, ⬆️Ig).
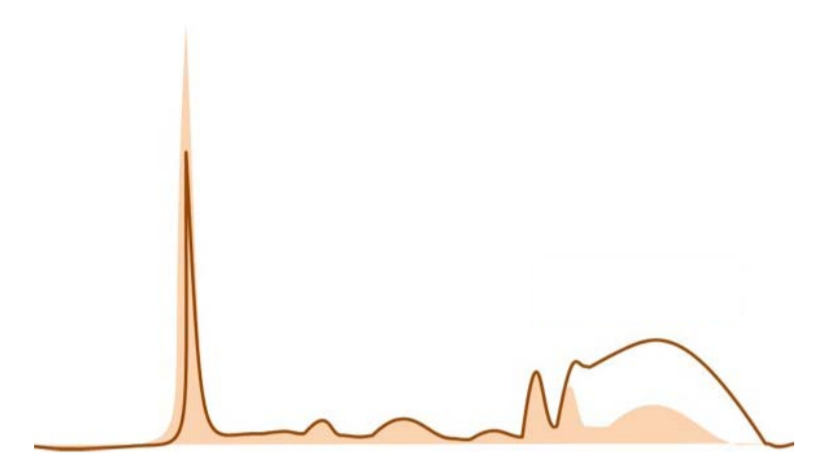
12/ Case #4:
What combination of pathologies is this pattern compatible with?
What combination of pathologies is this pattern compatible with?
12/ What combination of pathologies is this pattern compatible with?
13/ Answer: SLE/cirrhosis
When faced with a gammapathy (large protein or gamma gap), identify if pattern is monoclonal or polyclonal.
When faced with a gammapathy (large protein or gamma gap), identify if pattern is monoclonal or polyclonal.
13/ Answer: SLE/cirrhosis
Broad-based peak in this case is suggestive of polyclonal gammapathy, a condition seen in both SLE and cirrhosis.
Broad-based peak in this case is suggestive of polyclonal gammapathy, a condition seen in both SLE and cirrhosis.
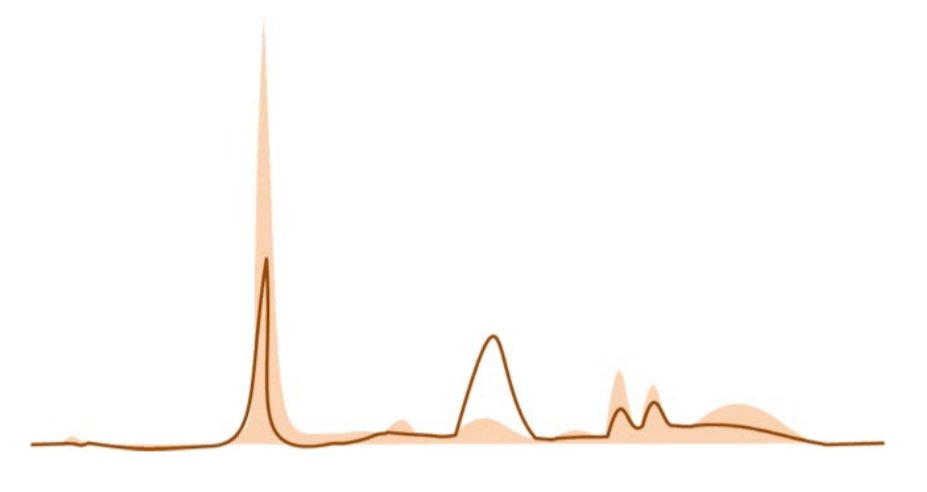
14/ Case #5:
What condition is the most likely diagnosis in this case?
What condition is the most likely diagnosis in this case?
14/ What condition is the most likely diagnosis in this case?
15/ Answer: IgG multiple myeloma
There is evidence of monoclonal gammapathy (narrow-based peak). M-protein level seems elevated and predominant in the γ region, mostly compatible with smoldering or active IgG MM.
IgA MGUS should cause a smaller spike shifted more to the left.
There is evidence of monoclonal gammapathy (narrow-based peak). M-protein level seems elevated and predominant in the γ region, mostly compatible with smoldering or active IgG MM.
IgA MGUS should cause a smaller spike shifted more to the left.
16/ Always interpret SPEP in clinical context.
If a plasma cell disorder is still suspected despite a normal SPEP, order a serum free light chain assay (sFLC). Up to 20% of plasma dyscrasias only produce light chains lost in urine. A normal sFLC ratio is 0.26-1.65 (⬆️ if GFR ⬇️).
If a plasma cell disorder is still suspected despite a normal SPEP, order a serum free light chain assay (sFLC). Up to 20% of plasma dyscrasias only produce light chains lost in urine. A normal sFLC ratio is 0.26-1.65 (⬆️ if GFR ⬇️).
Please share your thoughts/questions below.
Further reading:
Understanding and Interpreting Serum Protein Electrophoresis
aafp.org/afp/2005/0101/…
sciencedirect.com/topics/medicin…
Interprétation de l’électrophorèse
des protéines sériques. (in French)
fmc-tourcoing.org/new/wp-content…
Interesting cases:
ucsdlabmed.wikidot.com/chapter-7-labo…
Understanding and Interpreting Serum Protein Electrophoresis
aafp.org/afp/2005/0101/…
sciencedirect.com/topics/medicin…
Interprétation de l’électrophorèse
des protéines sériques. (in French)
fmc-tourcoing.org/new/wp-content…
Interesting cases:
ucsdlabmed.wikidot.com/chapter-7-labo…