
⚠️BREAKING: huge Chloroquine and Hydroxychloroquine study of 96,000 patients at 671 hospitals found:
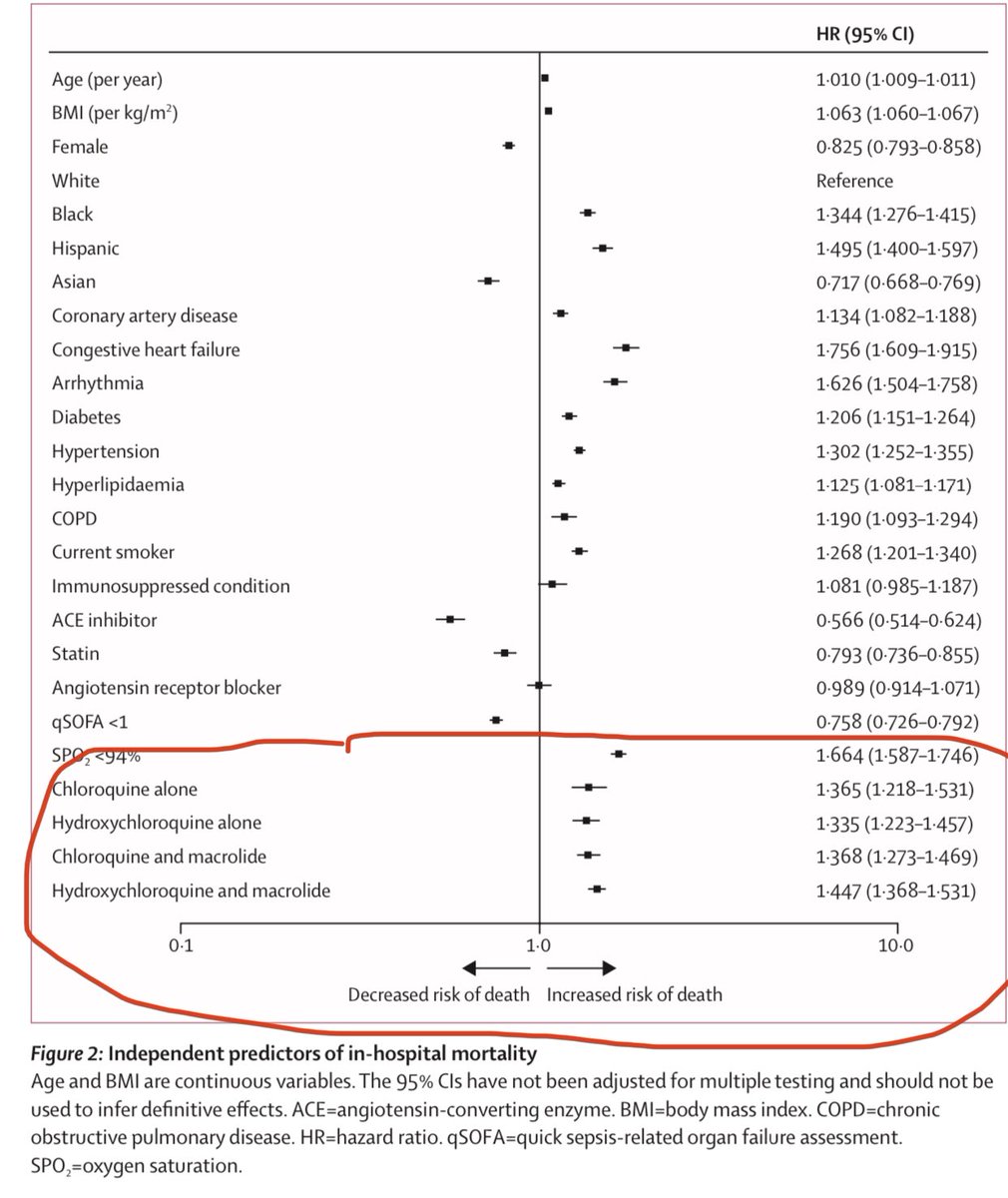
📌Increased risk of DEATH by 33-45%
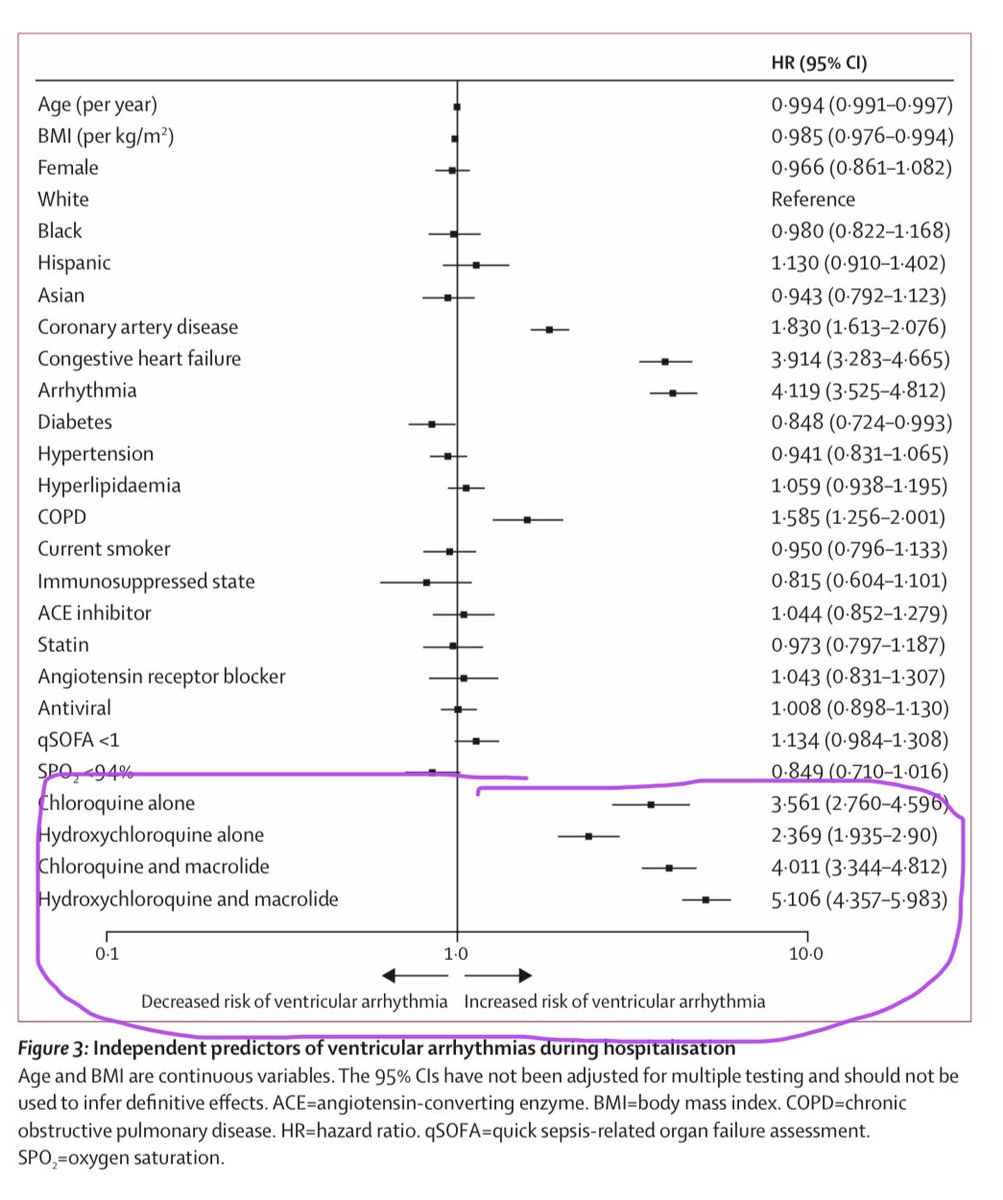
📌Increased risk of ventricular arrhythmia by 2.3x to 5x.
📌Not a trial but a large longitudinal study.
🧵#COVID19 washingtonpost.com/health/2020/05…
📌Increased risk of DEATH by 33-45%
📌Increased risk of ventricular arrhythmia by 2.3x to 5x.
📌Not a trial but a large longitudinal study.
🧵#COVID19 washingtonpost.com/health/2020/05…
2) “It’s one thing not to have benefit, but this shows distinct harm,” said Eric Topol, a cardiologist and director of the Scripps Research Translational Institute. “If there was ever was hope for this drug, this is the death of it.” 🔥
3) Patients studied from existing patient registries (important because it was pre recorded). Patients all strictly given HCQ or CQ within 48 hours of #covid19 diagnosis after hospitalization. Excluded if delayed.
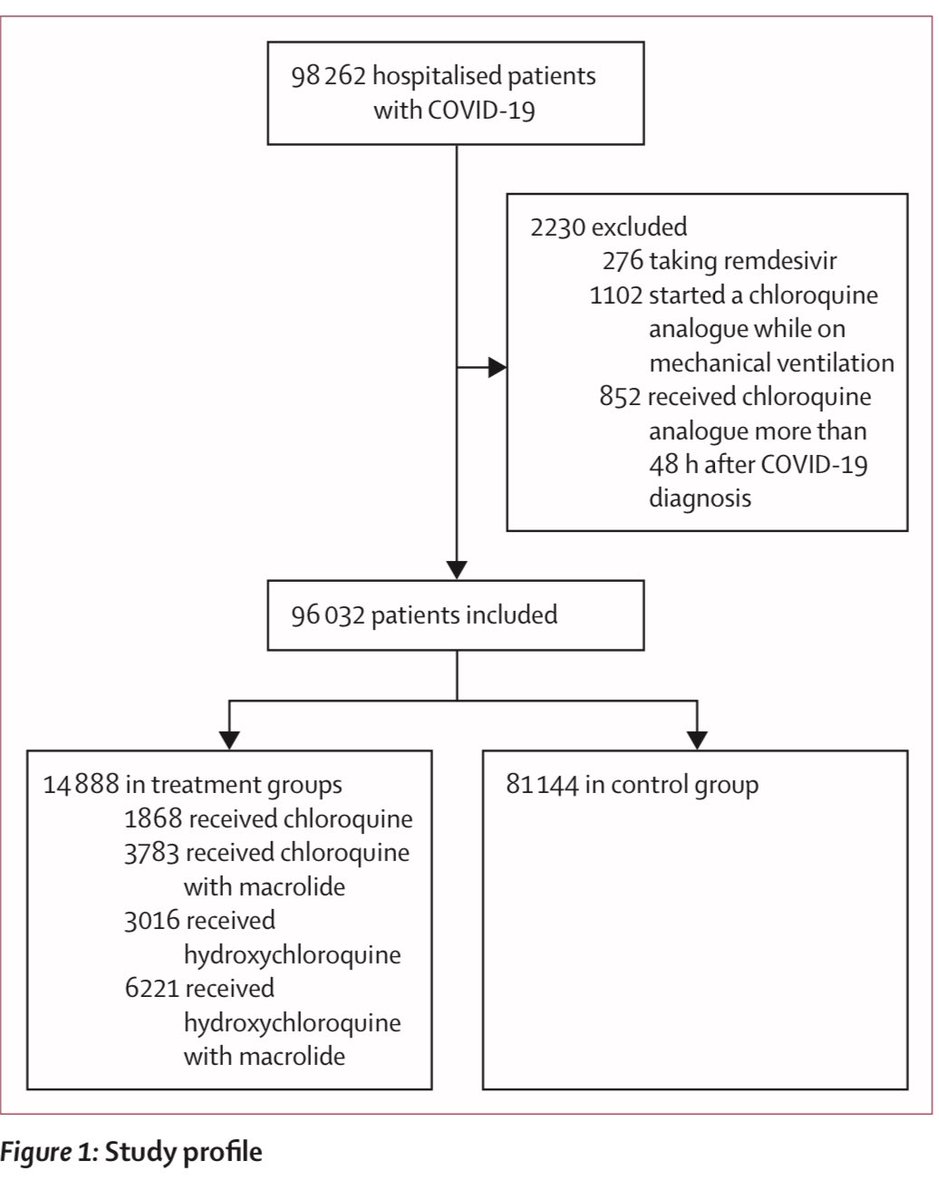
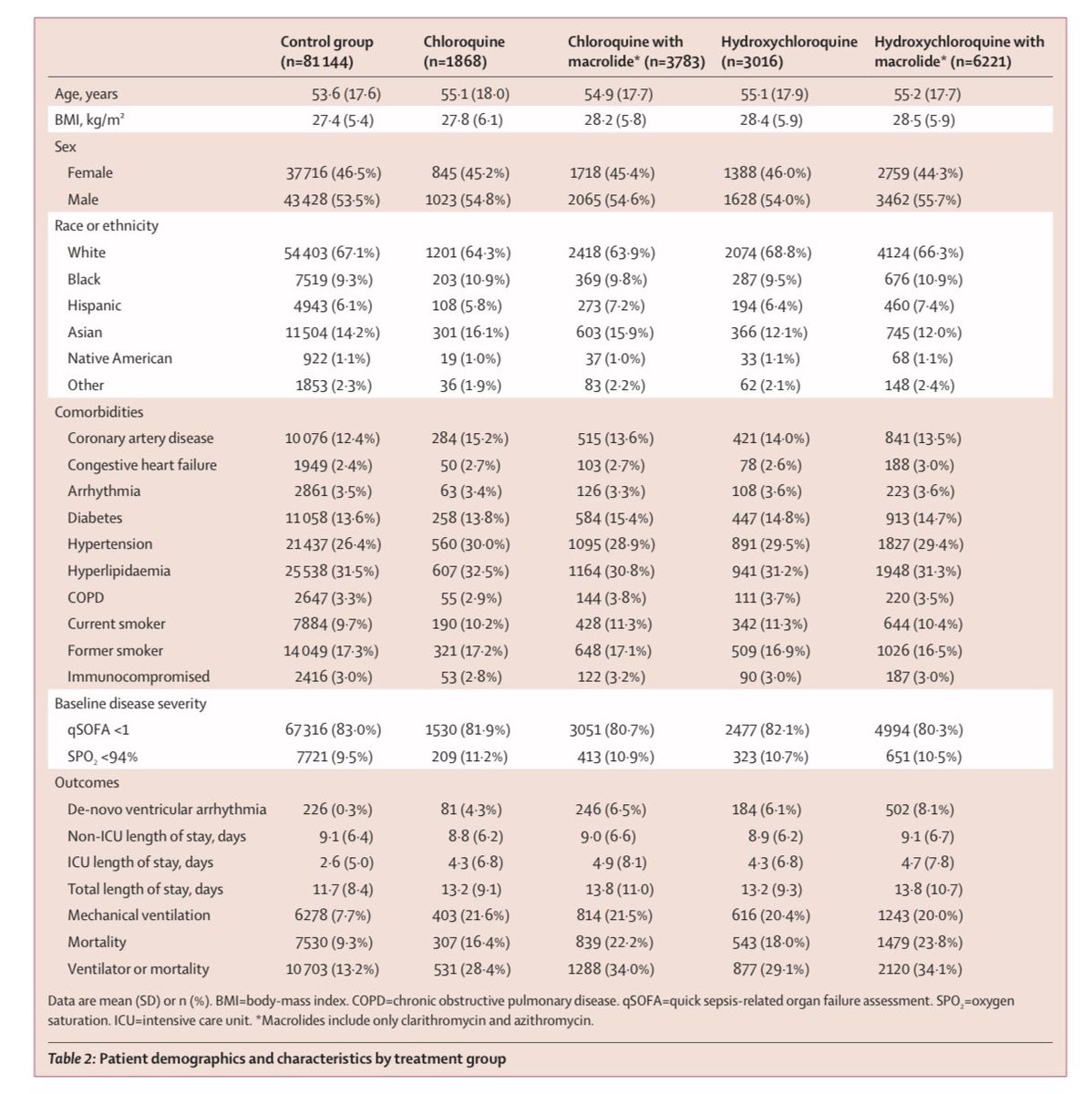
4) “The treatment groups included 1868 patients who were given chloroquine alone, 3016 given hydroxychloro- quine alone, 3783 given chloroquine w/ macrolide and 6221 given hydroxychloroquine and macrolide. The median time from hospitalisation to diagnosis of COVID-19 was 2 days.
5) “The mean daily dose and duration: chloroquine alone, 765 mg (SD 308) and 6·6 days (2·4); hydroxychloroquine alone, 596 mg (126) and 4·2 days (1·9); chloroquine w/ macrolide, 790 mg (320) and 6·8 days (2·5); and hydroxychloroquine w/ macrolide, 597 mg (128) and 4·3 days (2·0)”
6) “No significant between-group differences were found among baseline characteristics or comorbidities.”
➡️THIS IS QUITE REMARKABLE. Balanced means no baseline confounding. Akin to what you might see in a trial usually, except it wasn’t. Very reassuring.
➡️THIS IS QUITE REMARKABLE. Balanced means no baseline confounding. Akin to what you might see in a trial usually, except it wasn’t. Very reassuring.
7) “Analyses using propensity score matching by treatment group... indicated that associations between drug regimens and mortality, need for mechanical ventilation, length of stay, and the occurrence of de-novo ventricular arrhythmias were consistent with the primary analysis.”
8) “David Maron, director of preventive cardiology at the Stanford University School of Medicine, said that “these findings provide absolutely no reason for optimism that these drugs might be useful in the prevention or treatment of covid-19.”
9) Nearly 15,000 of the 96,000 patients in the analysis were treated with hydroxychloroquine or chloroquine alone or in combination with a type of antibiotics known as a macrolide, such as azithromycin, within 48 hours of their diagnosis.
10) The mean age was 54 years, and 53 percent were men. Those who were on mechanical ventilators or who received remdesivir, an antiviral drug made by Gilead Sciences that has shown promise in decreasing recovery times, were excluded.
11) For those given hydroxychloroquine, there was 34% increase in risk of mortality & 137% increased risk of serious heart arrhythmias. For those receiving hydroxychloroquine +antibiotic — there was 45% increased risk of death & 411% increased risk of serious heart arrhythmias.
12) “Those given chloroquine had a 37% increased risk of death and a 256% increased risk of serious heart arrhythmias. For those taking chloroquine and an antibiotic, there was a 37% increased risk of death and a 301% increased risk of serious heart arrhythmias.”
13) Clarification of “increased risk” nomenclature: hazard ratio of 5.0 denotes “inc risk by 5x” (drug user risk = 5*non user risk), or can also be described as a “400% increased risk of outcome”. In 1st post, I used the 5x language, which is same as 400% inc risk of X language.
14) Amazing that data came together from 671 hospitals across 6 continents!

15) In appendix, they also present results of a COMPOSITE endpoint if either mechanical ventilation or death (whichever came first in the Cox PH analysis). Results mostly same as the mortality endpoint, and even moderately stronger than death alone.

16) Other risk factors that stand out for higher risk of death:
📌Men
📌Adiposity (BMI)
📌Blacks and Hispanics vs White
📌Heart disease
📌Diabetes
📌Hypertension
📌High cholesterol
📌Smoking
📌⚠️Non-users of ACE inhibitor*
🔥⚠️Non-users of statins*
*Neat but need confirmation.
📌Men
📌Adiposity (BMI)
📌Blacks and Hispanics vs White
📌Heart disease
📌Diabetes
📌Hypertension
📌High cholesterol
📌Smoking
📌⚠️Non-users of ACE inhibitor*
🔥⚠️Non-users of statins*
*Neat but need confirmation.
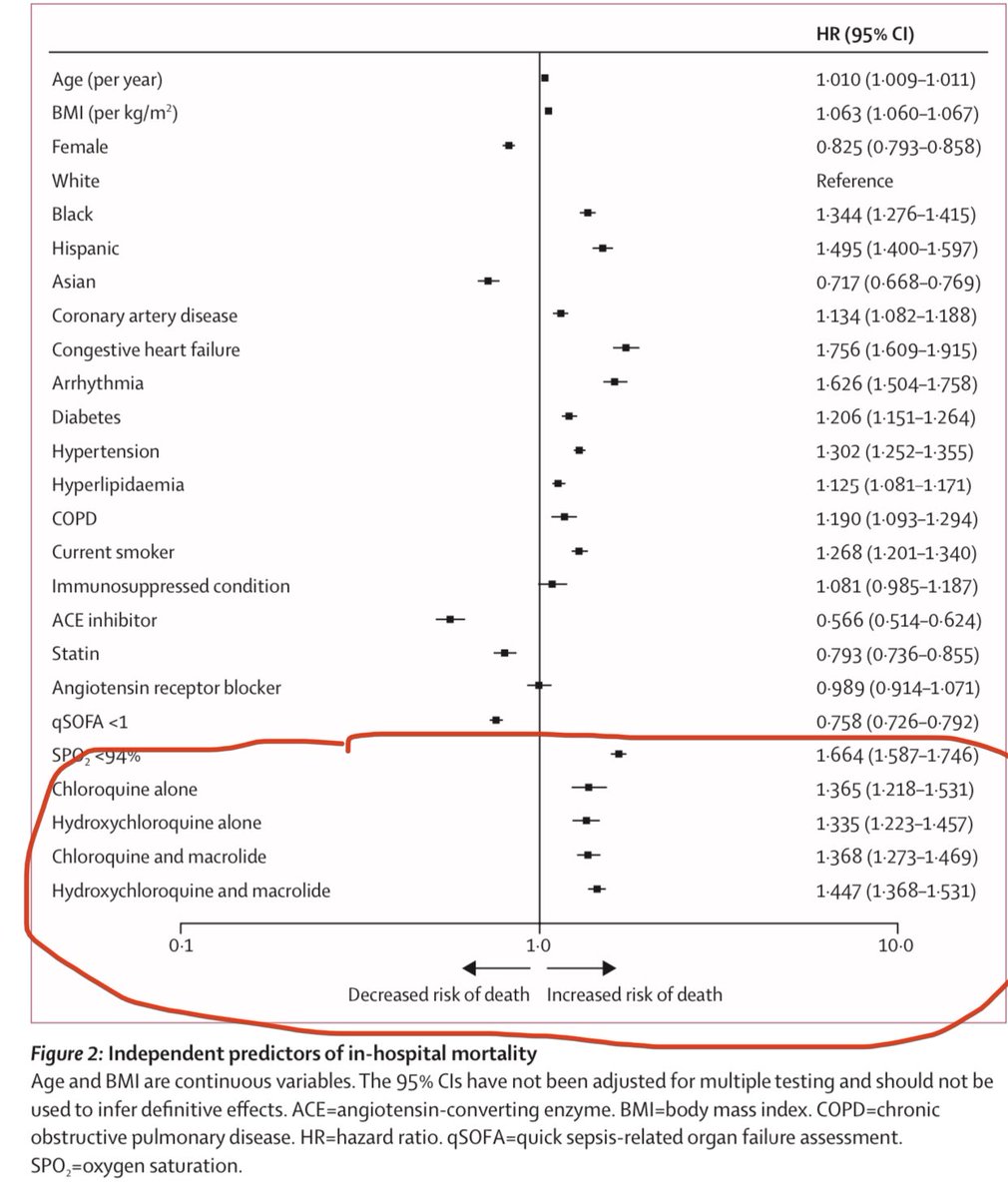
17) the strong findings of lower risk death for ACE inhibitors and statin users is interesting. But they area already drugs that are well known to lower risk of death. But do they lower even more among COVID patients? Unclear.
18) And racial data, I don’t want to overinterpret yet, because I don’t know if Blacks in Africa should be compared to whites in US/Europe. Prefer data on African Americans vs Whites in NA & African Europeans vs Whites in Europe w/in any continent. Same for Asians and Hispanics.
19) BOTTOMLINE: this study demonstrating CQ & HCQ increasing risk of death is an epic body of work representing amazing collaboration of 671 hospitals. Though not trial, it’s hospital registry data that is quite strong longitudinal design.
➡️ Do NOT take HCQ or CQ at this time!
➡️ Do NOT take HCQ or CQ at this time!
20) Full @TheLancet report available here: thelancet.com/lancet/article…. Great job @richardhorton1 and his editing team putting this out.
21) Does it definitely prove cause and effect? Not exactly. But keep in mind that the earliest studies back in 1950-1960s on smoking and lung cancer and heart disease were also longitudinal follow up studies that were observational. Smoking causality wasn’t proven until 1999! ...
22) ...had we waited to act on the overwhelming observational cohort evidence for smoking until 1999, untold millions would have been hurt or died. But the US Surgeon General put out landmark report implicating smoking and cancer in 1964 ➡️ & saved lives! cdc.gov/tobacco/data_s…
23) Like smoking, high blood pressure, high LDL, and more all were predicted to cause heart disease/death decades before their causality were established in trials years later. But early action based on overwhelming observational cohort data saved lives. Let’s simply be prudent.

