
Spent the last several hours trying to make sense of ACCT-1 (remdesivir). Several people DMed me, asking why I haven't commented. Answer: I took yesterday off.
Design: Multicentre double-blind RCT remdesivir (up to 10 days) vs placebo.
Effort: Herculean--an amazing collaboration.
Design: Multicentre double-blind RCT remdesivir (up to 10 days) vs placebo.
Effort: Herculean--an amazing collaboration.
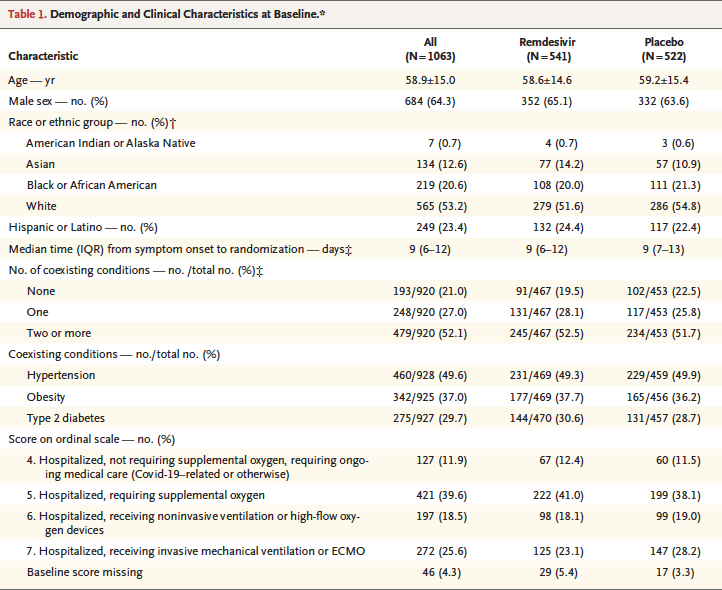
Population: hospitalized adults. 50% age 40-64. About 50% with pretty mild disease (see image 2 from Supplement). 

It's an adaptive trial. Many clinicians are unfamiliar with adaptive trials. Others just don't like them. Because they feel treif (i.e. not kosher): the definitive review IMHO is from @DLBHATTMD and Cyrus Mehta (ncbi.nlm.nih.gov/pubmed/27406349)

Initially (Feb), 1o outcome was % subjects reporting each severity rating on 7pt scale at D15 (n=394). In March, it was % used an 8pt ordinal scale (n=440), and then April 16, 1o outcome was "time to recovery" (n=572)--outcome not prev even a secondary outcome. Apr. 23 (n=800).
As indicated in the text, this change was made at the suggestion of trial statisticians, who noted that D15 status was less informative than "time to recovery" based on emerging information on the protracted nature of the disease.
I want to point out that the change from 7pt to 8pt scale was to divide "hospitalized, not requiring O2" into 5) requiring ongoing medical care and 6) no longer requires medical care.
As you know, the study was halted shortly after the "time to recovery" became the 1o outcome.
As you know, the study was halted shortly after the "time to recovery" became the 1o outcome.
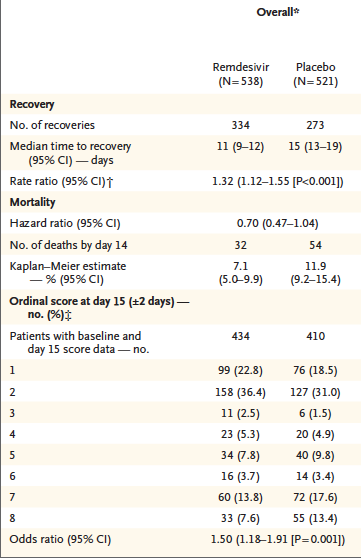
Just give us the goods already! Overall, there seems to be some improvement in all-comers. In particular, shortened time to recovery, possibly fewer deaths.

But for the sicker patients at baseline, remdesivir is of no benefit.
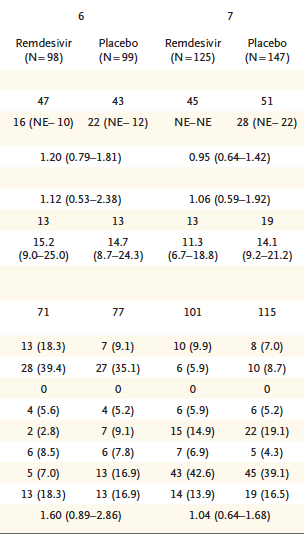


So who benefits? Well, maybe its the less sick patients: they seem to get out earlier. I am most impressed, however, with the difference in deaths at D14 in baseline score of 5 (hospitalized, requiring supplemental O2)


Finally, when you look at the overall data, it does seem to "favour" remdesivir. So it is a no-brainer, right--we should just give it?

I dunno. The one thing I do know, is--no reason to give to very sick patients: they don't benefit. Also, don't give to very well patient: they also don't benefit. But the 40% or so of patients on O2 who you've admitted--I think remdesivir should be given based on what we know.
I'm a skeptic with all new Rx. It's not the best treatment in the world, but would I want it if were admitted and on O2? Yes. If I were being ventilated? Nope. If I didn't need to be in hospital? Nope. Should they have stopped the trial early? No--we could have learned more.




