
Obsessive. Compulsive.🏀 coach. ID physician. Lots of XX chromosomes in my life. Fitness. No pharma conflicts.






 2. We are behind the UK, US, France, Germany, India and Japan on a national strategy.
2. We are behind the UK, US, France, Germany, India and Japan on a national strategy.
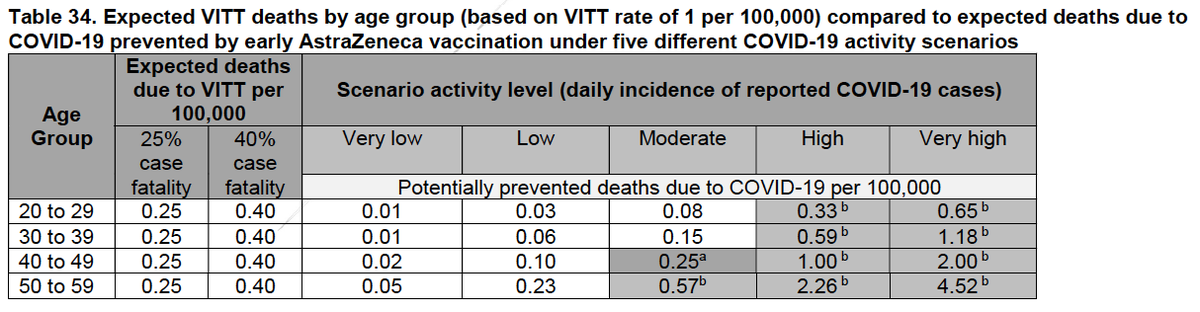 With this modeling, it makes clear sense to give AZ vs. waiting for age 50-69 in a moderate incidence setting, and for all ages in high incidence setting.
With this modeling, it makes clear sense to give AZ vs. waiting for age 50-69 in a moderate incidence setting, and for all ages in high incidence setting.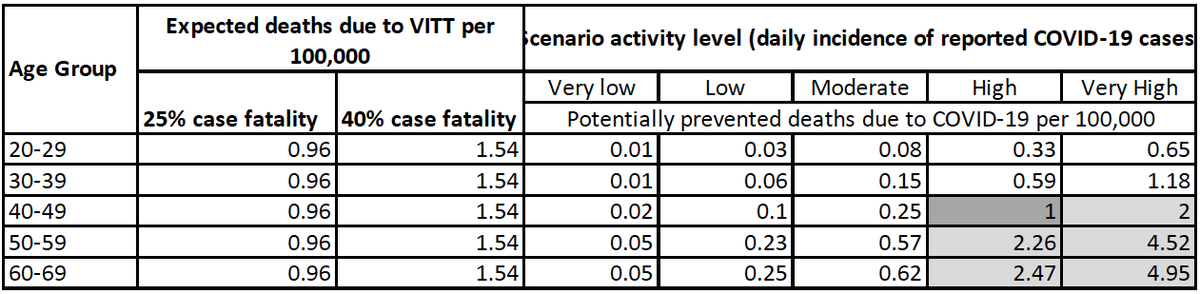

 It all hinges on the estimates of VITT. Yesterday @COVIDSciOntario posted a VITT brief covid19-sciencetable.ca/sciencebrief/v… that gave updated estimates of risk: 1:26 000 to 1:127 000 (as opposed to govt doc using 1:100-250K), and I believe ours is the most accurate estimate of risk of VITT.
It all hinges on the estimates of VITT. Yesterday @COVIDSciOntario posted a VITT brief covid19-sciencetable.ca/sciencebrief/v… that gave updated estimates of risk: 1:26 000 to 1:127 000 (as opposed to govt doc using 1:100-250K), and I believe ours is the most accurate estimate of risk of VITT.


 2. A huge difference is ICU capacity. In mid-December, we had around 276 patients with COVID in ICUs, and around 181 on ventilators.
2. A huge difference is ICU capacity. In mid-December, we had around 276 patients with COVID in ICUs, and around 181 on ventilators. 





 This is the ExCUSE (Examples of Canada, US, and Europe) approach. The govt. released their new plan predicated on this thinking. If I were to bet, it was conceived over 6 weeks ago (i.e. around Sept. 23). To remind you, this was ExCUSE total deaths and cases 6 weeks ago.
This is the ExCUSE (Examples of Canada, US, and Europe) approach. The govt. released their new plan predicated on this thinking. If I were to bet, it was conceived over 6 weeks ago (i.e. around Sept. 23). To remind you, this was ExCUSE total deaths and cases 6 weeks ago. 
