#LiverTwittIR #MedEd #Tweetorial
Management of post‐TIPS refractory Hepatic Encephalopathy (HE)
🟢 Definition
🟡 Prevention
🔵 Medical Rx
🔴 Endovascular approach
1/
Management of post‐TIPS refractory Hepatic Encephalopathy (HE)
🟢 Definition
🟡 Prevention
🔵 Medical Rx
🔴 Endovascular approach
1/
🟢 HE maybe:
Covert: Minimal or West haven Gr 1
Overt: West Haven Gr 2-4 which maybe episodic, recurrent (bouts within 6 mo) or persistent ( behavioral changes present with intermittent overt HE)
2/
Covert: Minimal or West haven Gr 1
Overt: West Haven Gr 2-4 which maybe episodic, recurrent (bouts within 6 mo) or persistent ( behavioral changes present with intermittent overt HE)
2/

Why does post-TIPS HE occur?
1.Shunting of blood away from liver- decreases 1st pass clearance of intestinal toxins (ammonia)
2. Upregulation of intestinal glutaminase activity- Increase ammonia production
1yr incidence 10-50%
New/ worsening 13-36%
Severe 1-3%
3/
1.Shunting of blood away from liver- decreases 1st pass clearance of intestinal toxins (ammonia)
2. Upregulation of intestinal glutaminase activity- Increase ammonia production
1yr incidence 10-50%
New/ worsening 13-36%
Severe 1-3%
3/
Several advances in #Irad in 2020, why does HE it still occur?
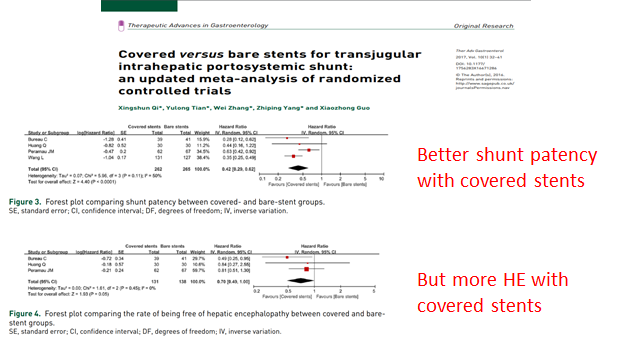
Early problems of TIPS instent narrowing due to open 'uncovered' stents - was actually protective from HE
Newer closed 'covered' stents allow robust flow- increasing chance of HE!
4/
Early problems of TIPS instent narrowing due to open 'uncovered' stents - was actually protective from HE
Newer closed 'covered' stents allow robust flow- increasing chance of HE!
4/
🟡 Prevention:
Patient selection: Age >65, previous HE, Child‐Pugh score >10 most robust predictors
Technical factors:
TIPS stent size: 8 mm better than 10 mm? Practice patterns and data all over.
5/
Patient selection: Age >65, previous HE, Child‐Pugh score >10 most robust predictors
Technical factors:
TIPS stent size: 8 mm better than 10 mm? Practice patterns and data all over.
5/
Portosystemic gradient after TIPS: reflects how much blood is being shunted across liver.
Keep gradient >5 to prevent HE
For variceal bleeding closer to 12, ascites closer to 8
Adjunctive variceal embolization during TIPS: more recent approach to obliterate non-TIPS shunts
6/
Keep gradient >5 to prevent HE
For variceal bleeding closer to 12, ascites closer to 8
Adjunctive variceal embolization during TIPS: more recent approach to obliterate non-TIPS shunts
6/
🔵 Medical Mx:
1. Identification and correction of precipitating event (i.e. new meds, dehydration, electrolyte disturbances, infection, GI bleeding,hepatic dysfunction), general support and adequate nutrition
2. Lactulose +- rifaximin
However 3-7% HE persists despite
7/
1. Identification and correction of precipitating event (i.e. new meds, dehydration, electrolyte disturbances, infection, GI bleeding,hepatic dysfunction), general support and adequate nutrition
2. Lactulose +- rifaximin
However 3-7% HE persists despite
7/
🔴 Endovascular Shunt reduction: decrease flow through TIPS by narrowing it. Various techniques(seperate tweetorial)
AIM: More flow to hepatocytes
Hepatofugal-away from liver
Hepatopedal-toward liver
Liver: HP
Cirrhosis: HF
TIPS: HP, Intrahep HF
Reduction: HP, Intrahep HP
8/
AIM: More flow to hepatocytes
Hepatofugal-away from liver
Hepatopedal-toward liver
Liver: HP
Cirrhosis: HF
TIPS: HP, Intrahep HF
Reduction: HP, Intrahep HP
8/

💥Dont take TIPS reduction lightly!
⬆️ Portal Htn, life threatening bleeding, mesenteric infarction
Important to establish clear relationship between TIPS n HE: short time interval, low PSG post TIPS, immediate deteriorating liver function
r/o other causes of Hep failure
9/
⬆️ Portal Htn, life threatening bleeding, mesenteric infarction
Important to establish clear relationship between TIPS n HE: short time interval, low PSG post TIPS, immediate deteriorating liver function
r/o other causes of Hep failure
9/
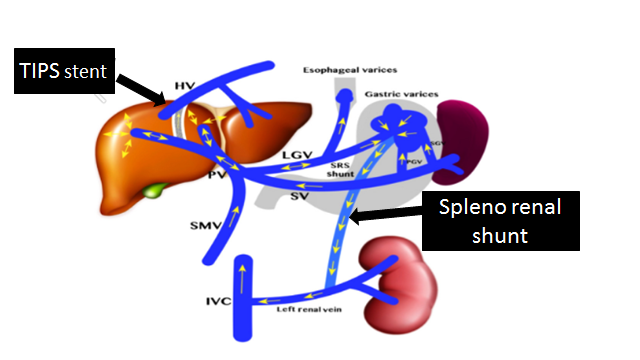
Competing shunts a double whammy for HE!
Variceal shunts and splenorenal shunts create a 'flow steal' phenomenon by shunting blood into systemic circulation even while TIPS continues shunting into systemic.
Important to recognize- easily treatable by #Irad embolization!
10/
Variceal shunts and splenorenal shunts create a 'flow steal' phenomenon by shunting blood into systemic circulation even while TIPS continues shunting into systemic.
Important to recognize- easily treatable by #Irad embolization!
10/
Take home points: