1/19
Why does cryptococcal meningitis cause such severe elevations in intracranial pressure (ICP)?
I had always accepted this as clinical fact without knowing the reason.
#tweetorial #medtwitter
Why does cryptococcal meningitis cause such severe elevations in intracranial pressure (ICP)?
I had always accepted this as clinical fact without knowing the reason.
#tweetorial #medtwitter
2/
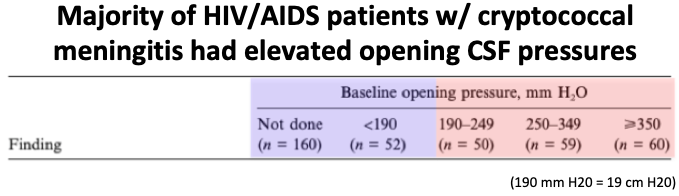
First we need to establish that cryptococcal meningitis is indeed associated w/ elevated ICP (>20 cm H20).
✅ 50-70% of HIV-infected patients with cryptococcal meningitis do present w/ increased ICP (less commonly in immunocompetent patients).
pubmed.ncbi.nlm.nih.gov/10619732
First we need to establish that cryptococcal meningitis is indeed associated w/ elevated ICP (>20 cm H20).
✅ 50-70% of HIV-infected patients with cryptococcal meningitis do present w/ increased ICP (less commonly in immunocompetent patients).
pubmed.ncbi.nlm.nih.gov/10619732
3/
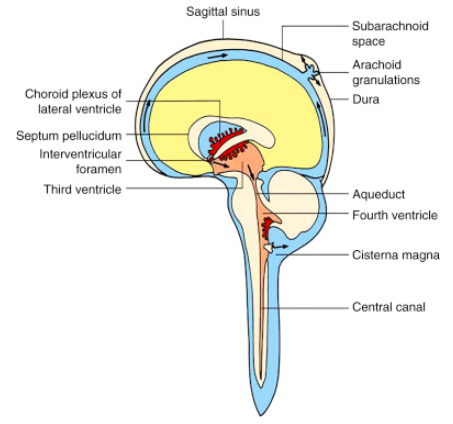
Next let's review cerebrospinal fluid (CSF) flow.
🔹 CSF is made by the choroid plexus, flows through the ventricles, and drains to the subarachnoid space.
🔹 It's then reabsorbed into the blood through arachnoid granulations along venous sinuses.
sciencedirect.com/topics/neurosc…
Next let's review cerebrospinal fluid (CSF) flow.
🔹 CSF is made by the choroid plexus, flows through the ventricles, and drains to the subarachnoid space.
🔹 It's then reabsorbed into the blood through arachnoid granulations along venous sinuses.
sciencedirect.com/topics/neurosc…
4/
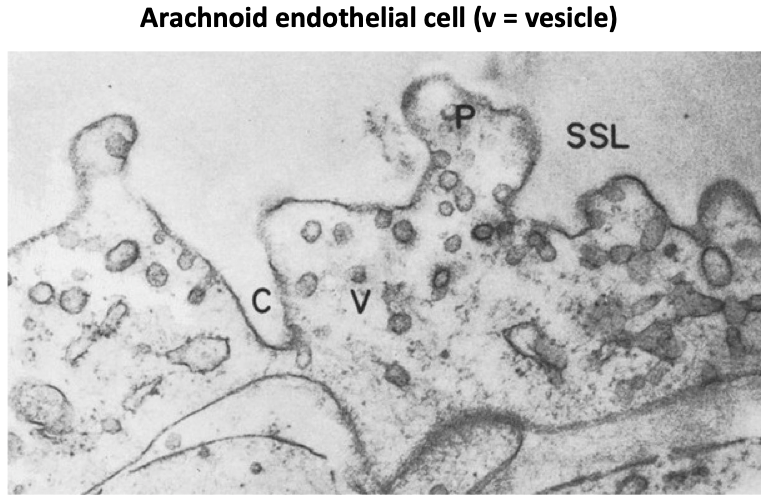
Endothelial cells associated w/ the arachnoid granulations form part of the blood brain barrier.
CSF returns to the blood across this barrier by way of transport in large intracellular vacuoles and smaller vesicles.
We'll return to these soon.
pubmed.ncbi.nlm.nih.gov/5825610/
Endothelial cells associated w/ the arachnoid granulations form part of the blood brain barrier.
CSF returns to the blood across this barrier by way of transport in large intracellular vacuoles and smaller vesicles.
We'll return to these soon.
pubmed.ncbi.nlm.nih.gov/5825610/
5/
Bacterial meningitis also elevates ICP, ❓due to inflammatory damage to the arachnoid granulations.
This is understandable as the CSF in bacterial meningitis is markedly inflamed and full of leukocytes (>1000 cells/microL)...
pubmed.ncbi.nlm.nih.gov/8416268/
Bacterial meningitis also elevates ICP, ❓due to inflammatory damage to the arachnoid granulations.
This is understandable as the CSF in bacterial meningitis is markedly inflamed and full of leukocytes (>1000 cells/microL)...
pubmed.ncbi.nlm.nih.gov/8416268/
6/
Conversely, with cryptococcus the CSF is often NOT inflamed (e.g. <50 leukocytes/microL) or at least significantly less inflamed than from bacterial meningitis.
So what about cryptococcal infection gives a predilection for elevated ICP?
pubmed.ncbi.nlm.nih.gov/15172774/
Conversely, with cryptococcus the CSF is often NOT inflamed (e.g. <50 leukocytes/microL) or at least significantly less inflamed than from bacterial meningitis.
So what about cryptococcal infection gives a predilection for elevated ICP?
pubmed.ncbi.nlm.nih.gov/15172774/
7/
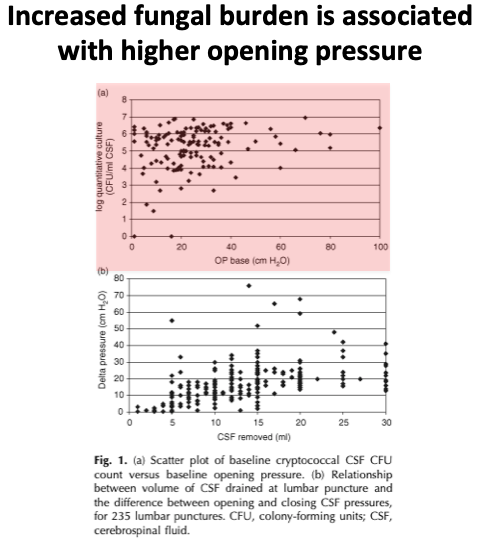
One clue may be the relationship between CSF opening pressure and fungal burden.
⚡️ It turns out that higher numbers of fungal organisms in the CSF is associated with higher opening pressures.
pubmed.ncbi.nlm.nih.gov/19279443/
One clue may be the relationship between CSF opening pressure and fungal burden.
⚡️ It turns out that higher numbers of fungal organisms in the CSF is associated with higher opening pressures.
pubmed.ncbi.nlm.nih.gov/19279443/
8/
This suggests that there's something about the cryptococcus organism that predisposes to ⬆️ ICP.
This suggests that there's something about the cryptococcus organism that predisposes to ⬆️ ICP.
9/
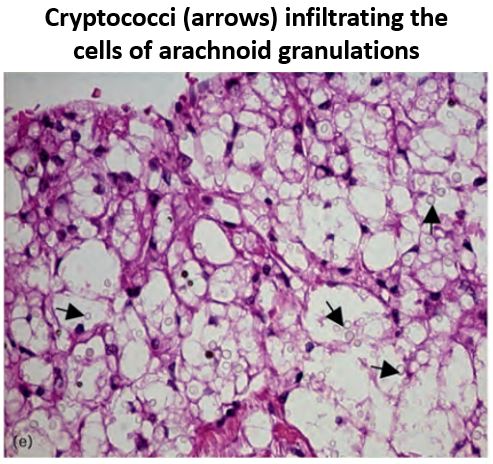
To find out what that "something" is, let's examine the arachnoid granulations histologically:
There were 2 notable findings w/ cryp. meningitis:
- Cryptococci infiltrated the granulations
- Vesicles and vacuoles were full of fungi (instead of CSF)
pubmed.ncbi.nlm.nih.gov/19952714/
To find out what that "something" is, let's examine the arachnoid granulations histologically:
There were 2 notable findings w/ cryp. meningitis:
- Cryptococci infiltrated the granulations
- Vesicles and vacuoles were full of fungi (instead of CSF)
pubmed.ncbi.nlm.nih.gov/19952714/
10/
Disruption of the arachnoid granulations, and mechanical blockage of CSF transport, seems to be the problem.
But other forms of fungal meningitis (eg histoplasmosis) aren't classically associated w/ raised ICP ncbi.nlm.nih.gov/pmc/articles/P…
What's different about cryptococcus?
Disruption of the arachnoid granulations, and mechanical blockage of CSF transport, seems to be the problem.
But other forms of fungal meningitis (eg histoplasmosis) aren't classically associated w/ raised ICP ncbi.nlm.nih.gov/pmc/articles/P…
What's different about cryptococcus?
11/
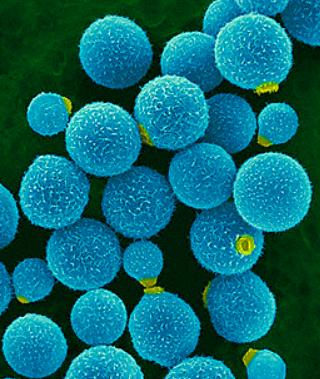
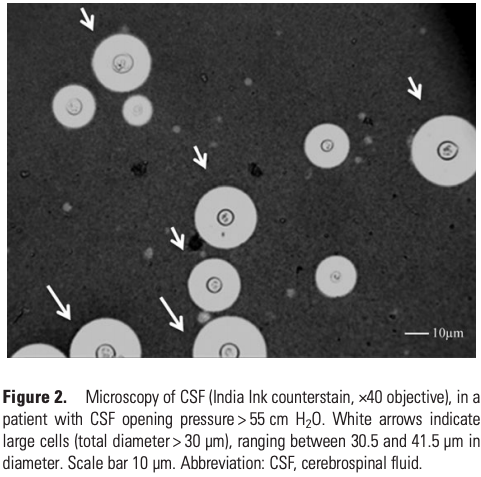
One unique feature of cryptococcus is the large size of the fungus itself.
Cryptococcus (a yeast) is 30 um in diameter, much larger than other yeast such as candida (10 um) or histoplasma (4 um).
sciencedirect.com/science/articl…
One unique feature of cryptococcus is the large size of the fungus itself.
Cryptococcus (a yeast) is 30 um in diameter, much larger than other yeast such as candida (10 um) or histoplasma (4 um).
sciencedirect.com/science/articl…
12/
But even more fascinating, cryptococcus has a distinctive polysaccharide capsule that contributes to its size and virulence.
(Quick aside: shed capsule = the cryptococcal antigen that we test for clinically!)
pubmed.ncbi.nlm.nih.gov/23945372/
But even more fascinating, cryptococcus has a distinctive polysaccharide capsule that contributes to its size and virulence.
(Quick aside: shed capsule = the cryptococcal antigen that we test for clinically!)
pubmed.ncbi.nlm.nih.gov/23945372/
13/
There is actually compelling animal and human data suggesting that cryptococcus' capsule, and that capsule's characteristics, may be the main pathogenic factor contributing to elevated ICP...
There is actually compelling animal and human data suggesting that cryptococcus' capsule, and that capsule's characteristics, may be the main pathogenic factor contributing to elevated ICP...
14/
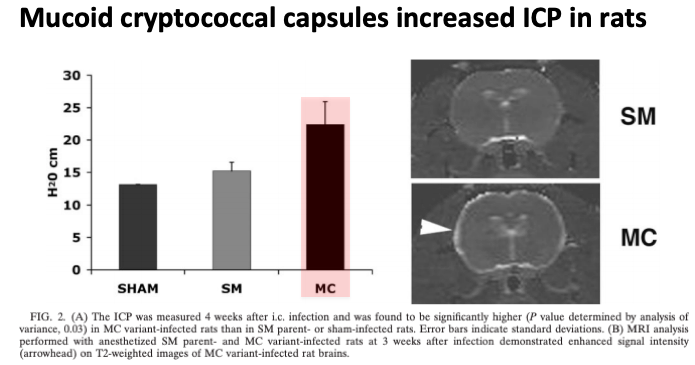
First, animal:
In rats infected w/ different strains of cryptococcus, only strains w/ a mucoid (vs smooth) capsule had ⬆️ ICP.
The authors theorized that ⬆️ viscosity of the mucoid capsule blocked CSF transport at the arachnoid granulations.
pubmed.ncbi.nlm.nih.gov/15731079/
First, animal:
In rats infected w/ different strains of cryptococcus, only strains w/ a mucoid (vs smooth) capsule had ⬆️ ICP.
The authors theorized that ⬆️ viscosity of the mucoid capsule blocked CSF transport at the arachnoid granulations.
pubmed.ncbi.nlm.nih.gov/15731079/
15/
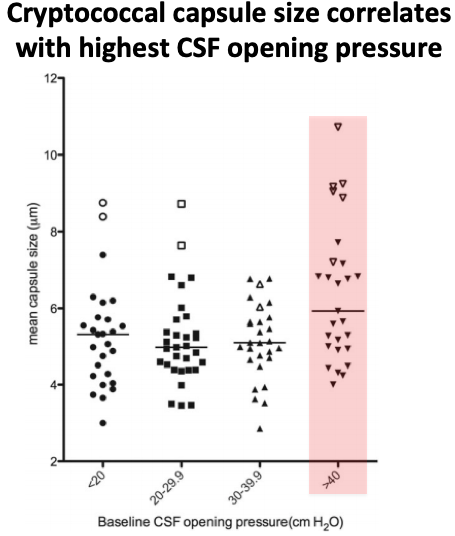
Next, human:
This study compared ICP and capsule size in HIV-associated cryptococcal meningitis.
Patients with the largest fungal capsules also had the highest CSF opening pressures, directly linking fungal capsule and elevated ICP.
pubmed.ncbi.nlm.nih.gov/23945372/
Next, human:
This study compared ICP and capsule size in HIV-associated cryptococcal meningitis.
Patients with the largest fungal capsules also had the highest CSF opening pressures, directly linking fungal capsule and elevated ICP.
pubmed.ncbi.nlm.nih.gov/23945372/
16/
Let's close with one final question.
Recall from tweet #4 that HIV-associated cryptococcal meningitis more commonly increases ICP than in immunocompetent patients.
Why would that be?
Let's close with one final question.
Recall from tweet #4 that HIV-associated cryptococcal meningitis more commonly increases ICP than in immunocompetent patients.
Why would that be?
17/
In patients w/ HIV, immune responses in the CSF are impaired.
This impaired immune response leads to higher fungal burdens, more capsule in the CSF, and more disruption of the arachnoid granulations.
pubmed.ncbi.nlm.nih.gov/15731079/
In patients w/ HIV, immune responses in the CSF are impaired.
This impaired immune response leads to higher fungal burdens, more capsule in the CSF, and more disruption of the arachnoid granulations.
pubmed.ncbi.nlm.nih.gov/15731079/
18/
B/c the mechanisms of ⬆️ ICP w/ bacterial and cryptococcal meningitis are different, there is a cool counterpoint w/ respect to inflammatory response:
Bacterial - ICP ⬆️ b/c of a robust inflammatory response
Cryptococcus - ICP ⬆️ b/c of a LACK of robust inflammatory response
B/c the mechanisms of ⬆️ ICP w/ bacterial and cryptococcal meningitis are different, there is a cool counterpoint w/ respect to inflammatory response:
Bacterial - ICP ⬆️ b/c of a robust inflammatory response
Cryptococcus - ICP ⬆️ b/c of a LACK of robust inflammatory response
19/
⚡️ Cryptococcal meningitis often increases ICP
⚡️ This results from a polysaccharide capsule (contributing to the fungus' large size) that blocks transport of CSF through the arachnoid granulations, raising ICP
⚡️ ⬆️ ICP is more common in HIV+ due to higher fungal burdens
⚡️ Cryptococcal meningitis often increases ICP
⚡️ This results from a polysaccharide capsule (contributing to the fungus' large size) that blocks transport of CSF through the arachnoid granulations, raising ICP
⚡️ ⬆️ ICP is more common in HIV+ due to higher fungal burdens