1/15
[How] does caffeine act as a diuretic?
I've long assumed that my morning cup of coffee directly results in my morning trip to the bathroom.
But, is it just the ingestion of fluid, or is there something specific about caffeine/coffee?
Grab a cup and let's find out.
[How] does caffeine act as a diuretic?
I've long assumed that my morning cup of coffee directly results in my morning trip to the bathroom.
But, is it just the ingestion of fluid, or is there something specific about caffeine/coffee?
Grab a cup and let's find out.

2/
First, a question.
Which of the following is characteristic of the diuretic effects of caffeine?
First, a question.
Which of the following is characteristic of the diuretic effects of caffeine?
3/
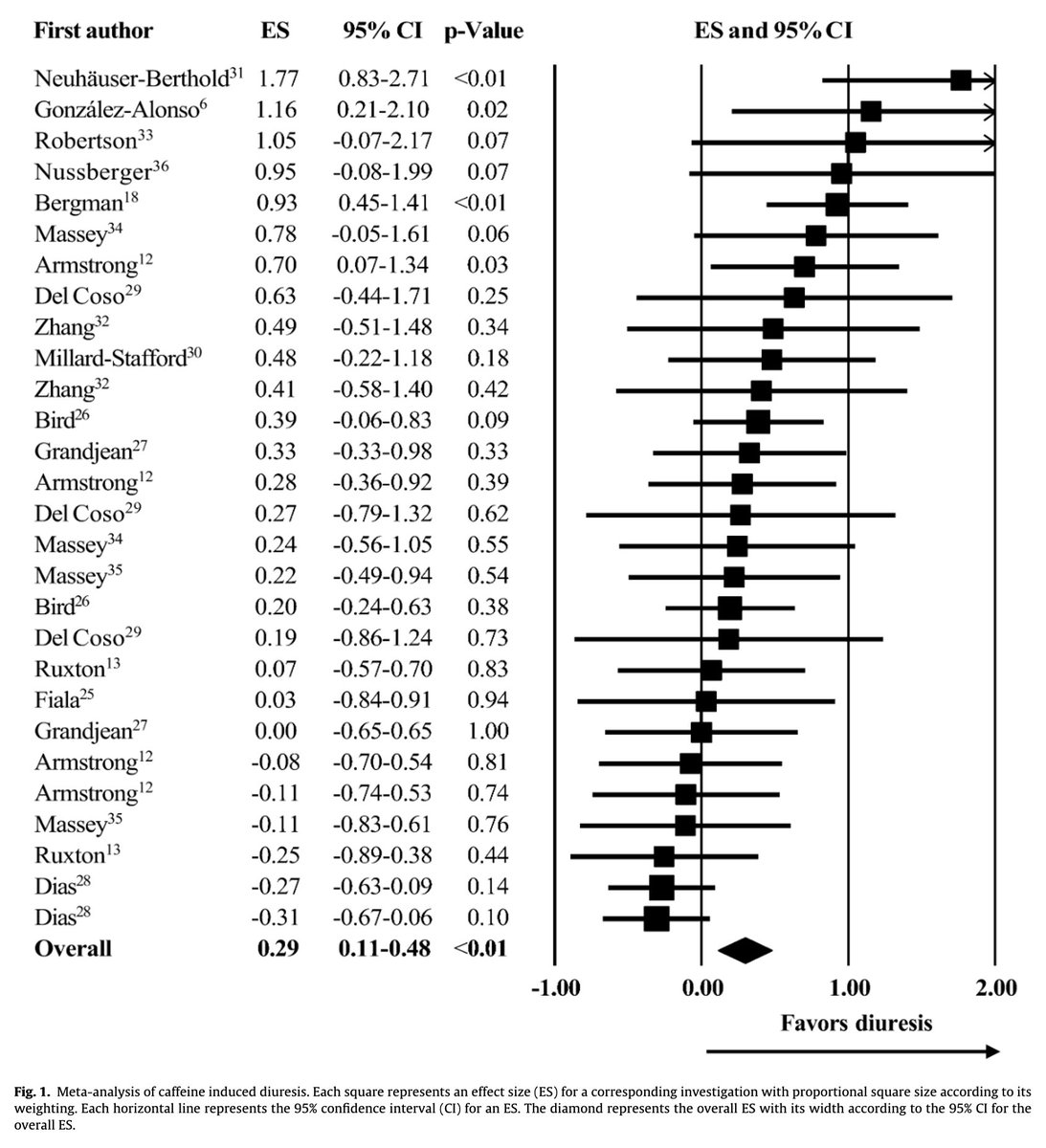
Before discussing potential mechanisms, let's establish that caffeine IS a diuretic.
One meta-analysis concluded that caffeine has a minor diuretic effect (~100 mL increase in urine volume).
But, there does seem to be an effect.
pubmed.ncbi.nlm.nih.gov/25154702/
Before discussing potential mechanisms, let's establish that caffeine IS a diuretic.
One meta-analysis concluded that caffeine has a minor diuretic effect (~100 mL increase in urine volume).
But, there does seem to be an effect.
pubmed.ncbi.nlm.nih.gov/25154702/
4/
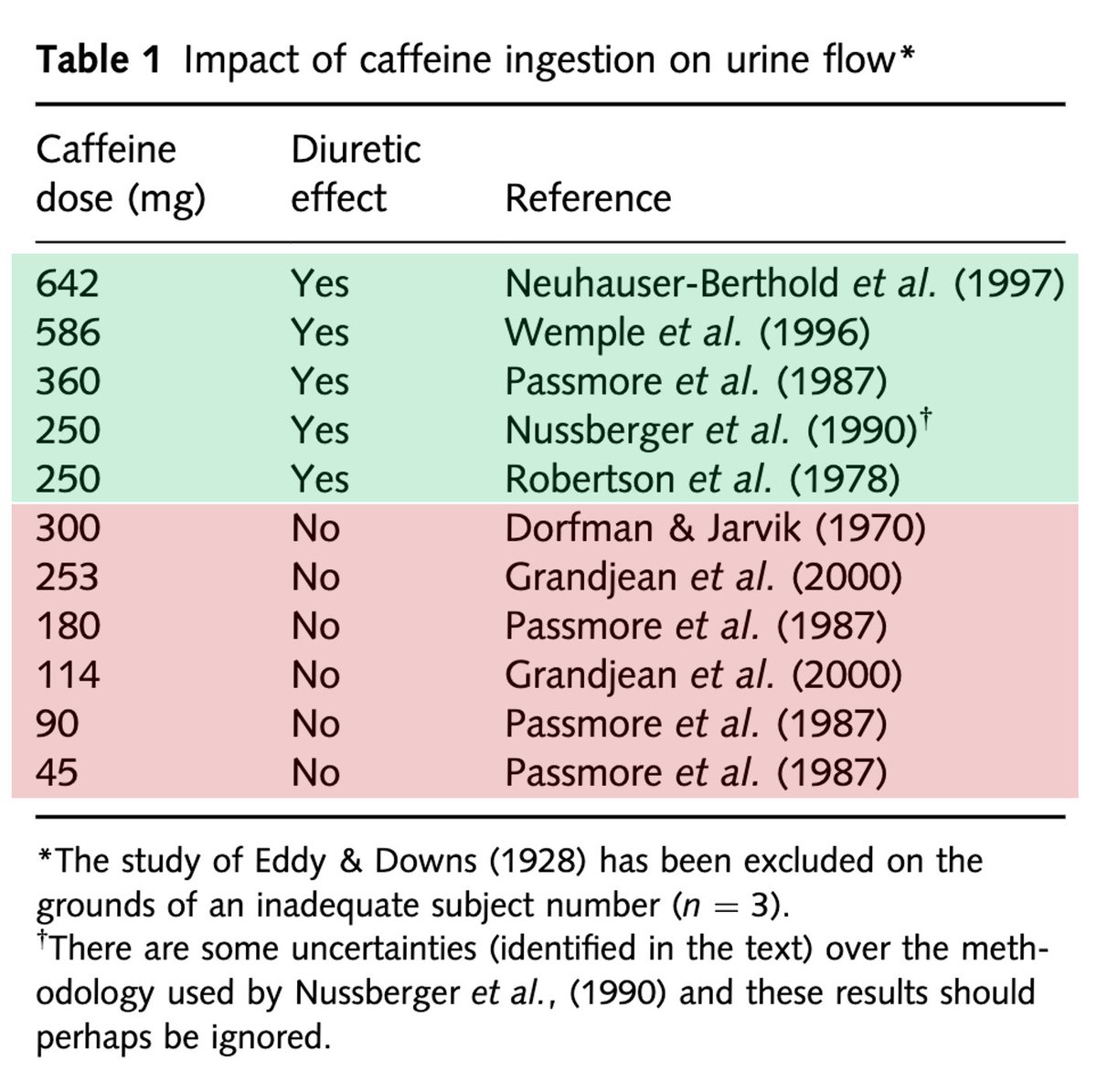
There are at least two observations when reviewing these studies:
🔹Higher doses of caffeine are required
🔹Tolerance develops (i.e., daily coffee drinkers are less likely to experience a diuresis)
There are at least two observations when reviewing these studies:
🔹Higher doses of caffeine are required
🔹Tolerance develops (i.e., daily coffee drinkers are less likely to experience a diuresis)
5/
While the exact cut-off at which caffeine exerts a diuretic effect is surely dependent on many factors, it seems that at least 300mg is required.
For reference, a grande coffee at Starbucks contains about 300mg of caffeine. A venti may be required.
pubmed.ncbi.nlm.nih.gov/19774754/
While the exact cut-off at which caffeine exerts a diuretic effect is surely dependent on many factors, it seems that at least 300mg is required.
For reference, a grande coffee at Starbucks contains about 300mg of caffeine. A venti may be required.
pubmed.ncbi.nlm.nih.gov/19774754/
6/
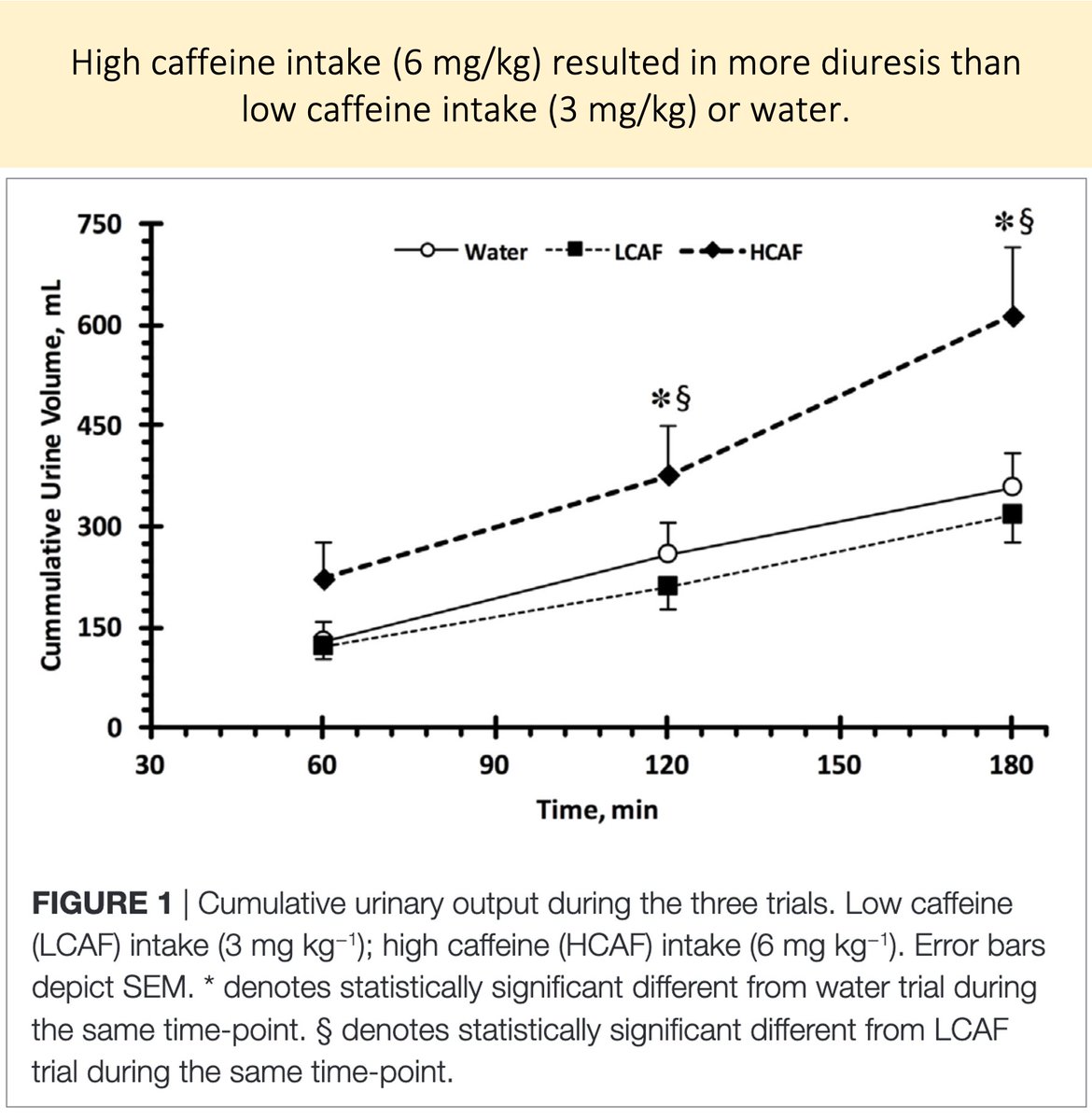
Tolerance appears to develops.
RCTs that show a diuretic effect often include a washout period.
For example, one study found increased urine output with high dose caffeine (~ what's in a venti Starbucks) AFTER a 24-hour period without caffeine.
pubmed.ncbi.nlm.nih.gov/28868290/
Tolerance appears to develops.
RCTs that show a diuretic effect often include a washout period.
For example, one study found increased urine output with high dose caffeine (~ what's in a venti Starbucks) AFTER a 24-hour period without caffeine.
pubmed.ncbi.nlm.nih.gov/28868290/
7/
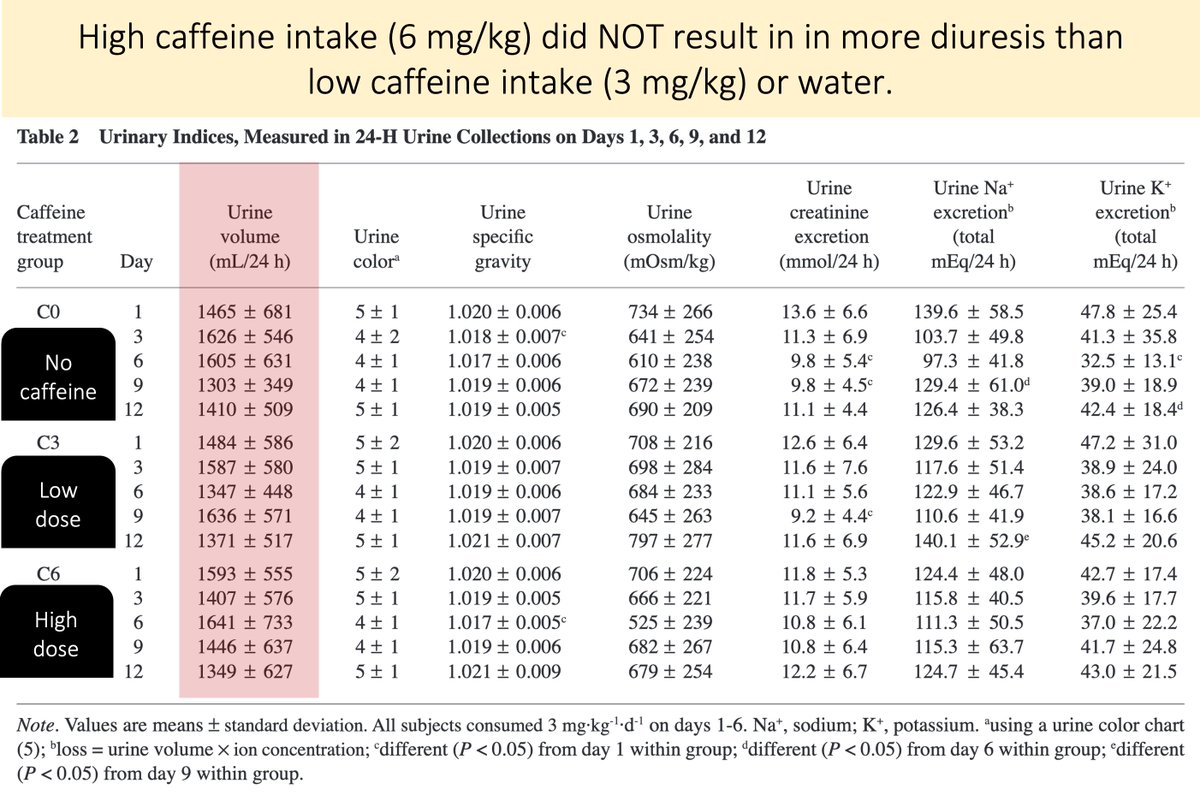
Studies that include participants who are daily users show less of an effect.
A study using the same high dose as in tweet 6 (i.e., 6mg/kg) found NO increase in urine volume.
One difference: all participants consumed 3mg/kg daily as a lead-in.
pubmed.ncbi.nlm.nih.gov/16131696/
Studies that include participants who are daily users show less of an effect.
A study using the same high dose as in tweet 6 (i.e., 6mg/kg) found NO increase in urine volume.
One difference: all participants consumed 3mg/kg daily as a lead-in.
pubmed.ncbi.nlm.nih.gov/16131696/
8/
Accepting that there is some diuretic effect, what is the mechanism?
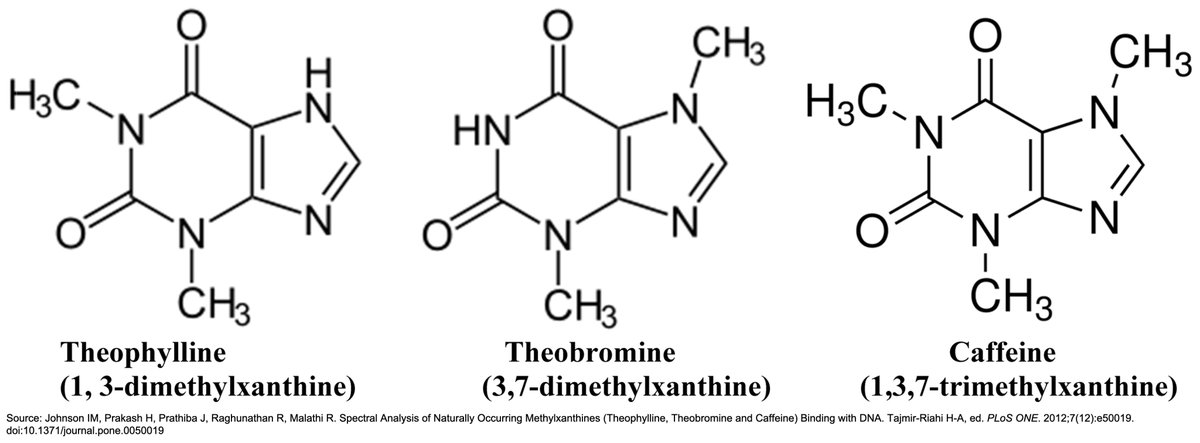
To understand the answer, recall that caffeine is a methylxanthine. And, like other methylxanthines (e.g., theophylline), it is a competitive inhibitor of adenosine receptors.
pubmed.ncbi.nlm.nih.gov/20859805/
Accepting that there is some diuretic effect, what is the mechanism?
To understand the answer, recall that caffeine is a methylxanthine. And, like other methylxanthines (e.g., theophylline), it is a competitive inhibitor of adenosine receptors.
pubmed.ncbi.nlm.nih.gov/20859805/
9/
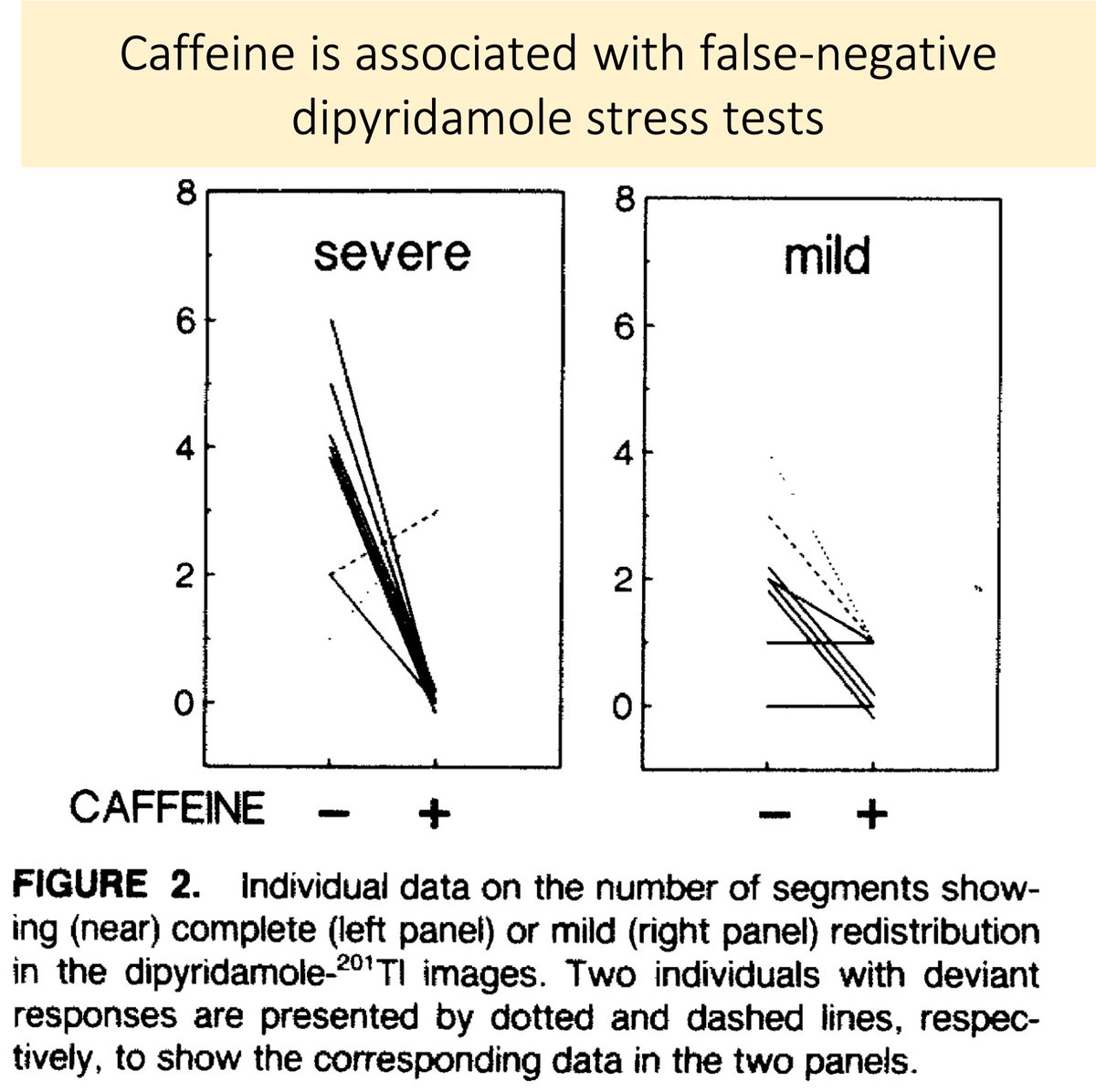
The competitive inhibition of adenosine receptors is the reason why caffeine is held prior to stress tests.
The idea: caffeine may lead to false-negative results via its blunting of adenosine-mediated vasodilation.
pubmed.ncbi.nlm.nih.gov/1869975/
The competitive inhibition of adenosine receptors is the reason why caffeine is held prior to stress tests.
The idea: caffeine may lead to false-negative results via its blunting of adenosine-mediated vasodilation.
pubmed.ncbi.nlm.nih.gov/1869975/
10/
Studies of knockout mice suggest that adenosine A1 receptors are required for the diuretic effect of methylxanthines, including caffeine.
Without these receptors, the mice didn't pee after caffeine ingestion (45mg/kg - a HUGE dose).
pubmed.ncbi.nlm.nih.gov/15590766/
Studies of knockout mice suggest that adenosine A1 receptors are required for the diuretic effect of methylxanthines, including caffeine.
Without these receptors, the mice didn't pee after caffeine ingestion (45mg/kg - a HUGE dose).
pubmed.ncbi.nlm.nih.gov/15590766/
11/
Additional studies suggest that caffeine (via adenosine A1 receptor antagonism) may affect the proximal tubule sodium/bicarbonate cotransporter.
This may be the "site" of caffeine's diuretic effect.
pubmed.ncbi.nlm.nih.gov/25925253/
Additional studies suggest that caffeine (via adenosine A1 receptor antagonism) may affect the proximal tubule sodium/bicarbonate cotransporter.
This may be the "site" of caffeine's diuretic effect.
pubmed.ncbi.nlm.nih.gov/25925253/
12/
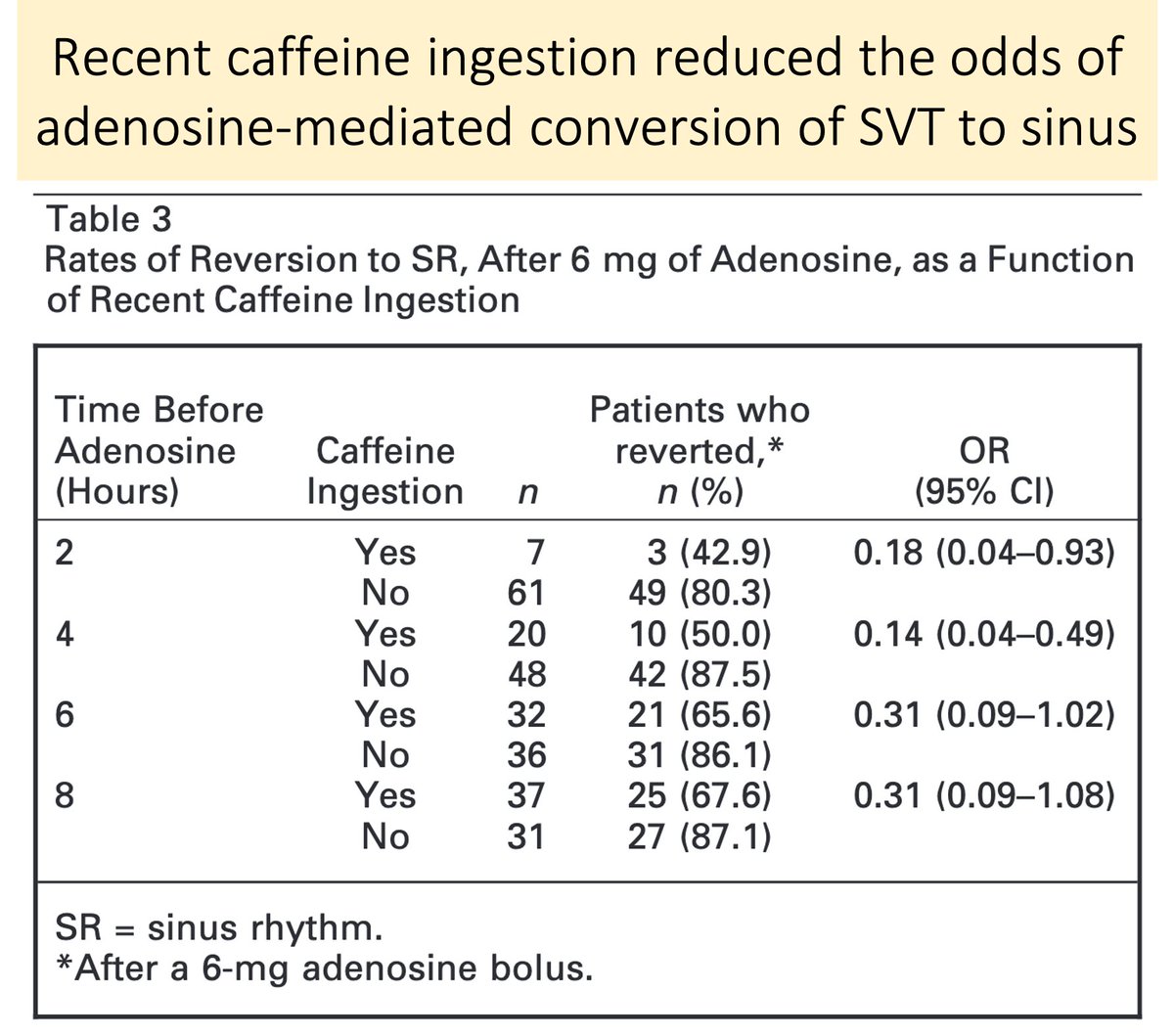
There are many cool clinical correlates that make use of caffeine's mechanism of action.
First, in patients with supraventricular tachycardia, the recent ingestion of caffeine reduces adenosine efficacy (by antagonizing its receptor).
pubmed.ncbi.nlm.nih.gov/20003123/
There are many cool clinical correlates that make use of caffeine's mechanism of action.
First, in patients with supraventricular tachycardia, the recent ingestion of caffeine reduces adenosine efficacy (by antagonizing its receptor).
pubmed.ncbi.nlm.nih.gov/20003123/
13/
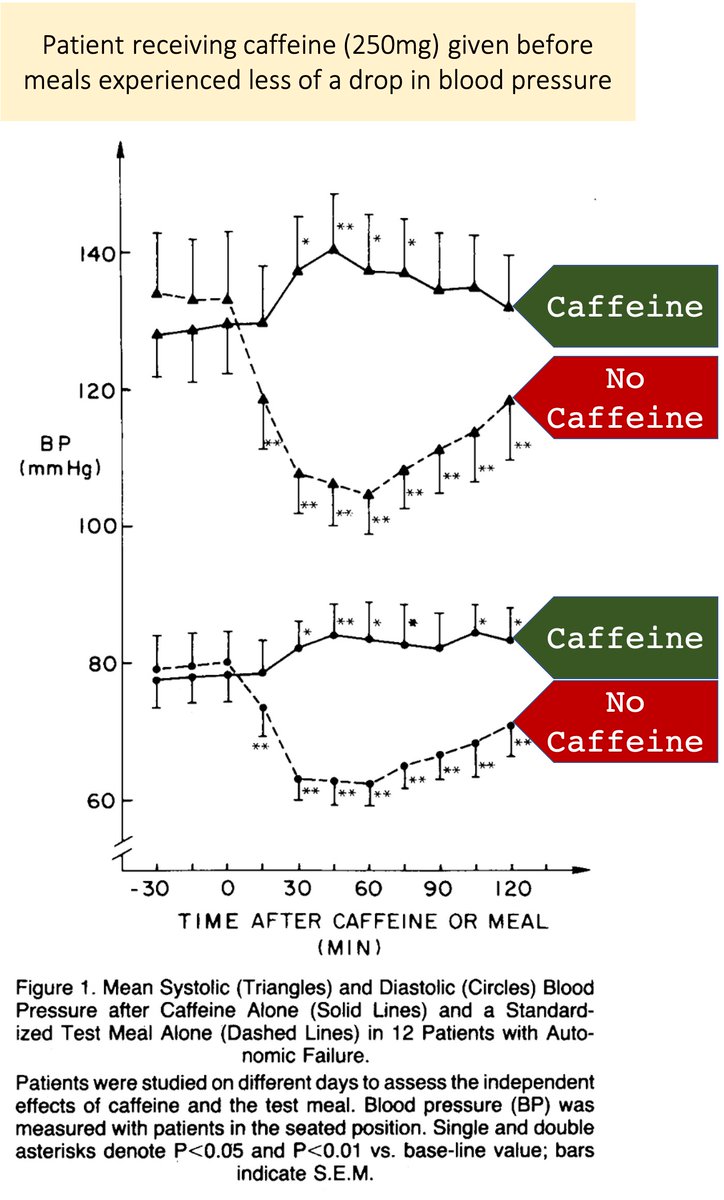
Given that adenosine is a vasodilator, one might suspect caffeine leads to vasoconstriction.
In fact, caffeine has been shown to combat postprandial hypotension!
And, caffeine withdrawal headaches likely result from adenosine-mediated vasodilation.
pubmed.ncbi.nlm.nih.gov/3894971/
Given that adenosine is a vasodilator, one might suspect caffeine leads to vasoconstriction.
In fact, caffeine has been shown to combat postprandial hypotension!
And, caffeine withdrawal headaches likely result from adenosine-mediated vasodilation.
pubmed.ncbi.nlm.nih.gov/3894971/
14/
Before closing, I'm curious. What is your experience with caffeine's purported diuretic effect?
Before closing, I'm curious. What is your experience with caffeine's purported diuretic effect?
15/15 [Summary]
☕️Caffeine is a methylxanthine
☕️Caffeine's diuretic effect:
▪️requires high doses (think Venti from Starbucks)
▪️is mitigated by daily use
▪️likely results from adenosine receptor antagonism in the proximal tubule
☕️I love coffee
☕️Caffeine is a methylxanthine
☕️Caffeine's diuretic effect:
▪️requires high doses (think Venti from Starbucks)
▪️is mitigated by daily use
▪️likely results from adenosine receptor antagonism in the proximal tubule
☕️I love coffee
For you @ETSshow