1/15
Why does alpha-1 antitrypsin deficiency (A1AT) cause liver disease (e.g. cirrhosis or hepatocellular carcinoma)?
I always assumed the mechanism was the same as for lung injury and emphysema, but it's not.
#tweetorial #medtwitter
Why does alpha-1 antitrypsin deficiency (A1AT) cause liver disease (e.g. cirrhosis or hepatocellular carcinoma)?
I always assumed the mechanism was the same as for lung injury and emphysema, but it's not.
#tweetorial #medtwitter
2/
Let's review the pathophys of A1AT:
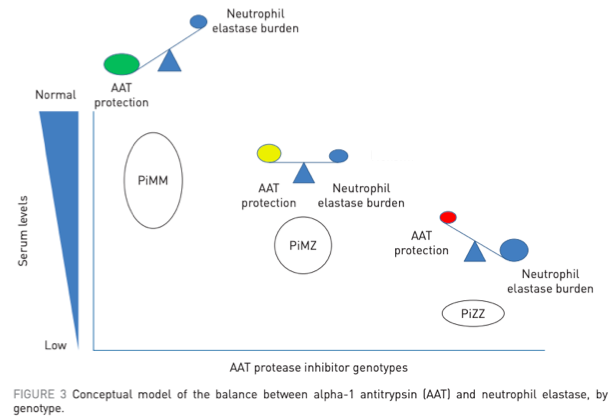
- Alpha-1 antitrypsin (AAT) is a protease inhibitor, made in the liver, targeting neutrophil elastase
- Mutated alleles lead to decreased production of AAT (MM = normal genotype, ZZ = most common variant in A1AT)
pubmed.ncbi.nlm.nih.gov/29070580/
Let's review the pathophys of A1AT:
- Alpha-1 antitrypsin (AAT) is a protease inhibitor, made in the liver, targeting neutrophil elastase
- Mutated alleles lead to decreased production of AAT (MM = normal genotype, ZZ = most common variant in A1AT)
pubmed.ncbi.nlm.nih.gov/29070580/
3/
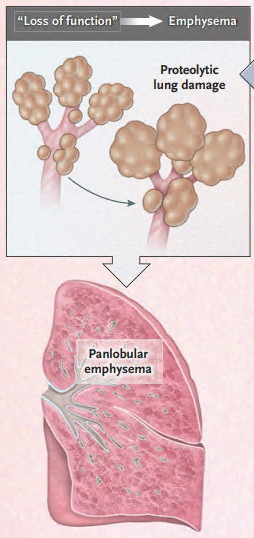
A1AT is most well known as an inherited cause of emphysema.
This occurs b/c of a "toxic loss of function" where elastase would normally be inhibited by AAT.
Loss of AAT production leads to uninhibited elastase activity and alveolar destruction.
pubmed.ncbi.nlm.nih.gov/32268028/
A1AT is most well known as an inherited cause of emphysema.
This occurs b/c of a "toxic loss of function" where elastase would normally be inhibited by AAT.
Loss of AAT production leads to uninhibited elastase activity and alveolar destruction.
pubmed.ncbi.nlm.nih.gov/32268028/
4/
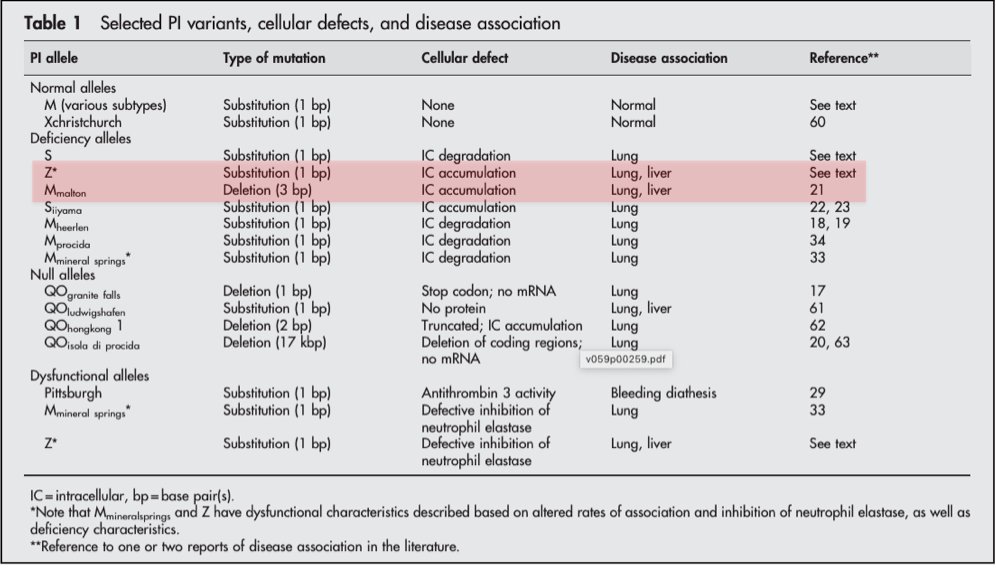
What about the mechanism of liver disease in A1AT?
One clue is that only some AAT mutations lead to liver disease: Z (genotype ZZ) + M-malton (and, rarely, S).
Z is the most common mutation in A1AT and has the strongest association w/ liver disease.
pubmed.ncbi.nlm.nih.gov/14985567/
What about the mechanism of liver disease in A1AT?
One clue is that only some AAT mutations lead to liver disease: Z (genotype ZZ) + M-malton (and, rarely, S).
Z is the most common mutation in A1AT and has the strongest association w/ liver disease.
pubmed.ncbi.nlm.nih.gov/14985567/
5/
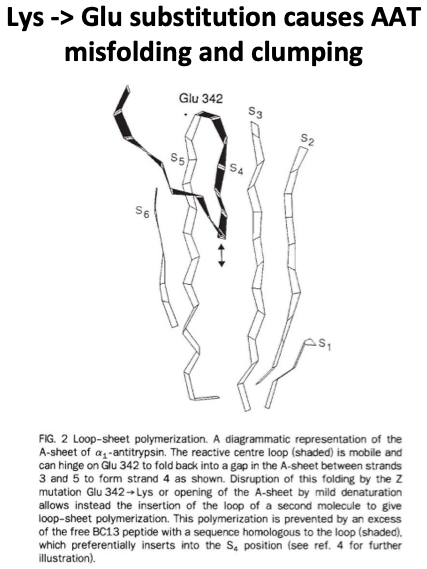
Next, let's learn the effects of the Z mutation to see why it can cause liver disease.
With Z, lysine substitutes for glutamic acid at a hinge point in AAT.
This causes protein misfolding/polymerization in the hepatocyte endoplasmic reticulum (ER).
pubmed.ncbi.nlm.nih.gov/1608473/
Next, let's learn the effects of the Z mutation to see why it can cause liver disease.
With Z, lysine substitutes for glutamic acid at a hinge point in AAT.
This causes protein misfolding/polymerization in the hepatocyte endoplasmic reticulum (ER).
pubmed.ncbi.nlm.nih.gov/1608473/
6/
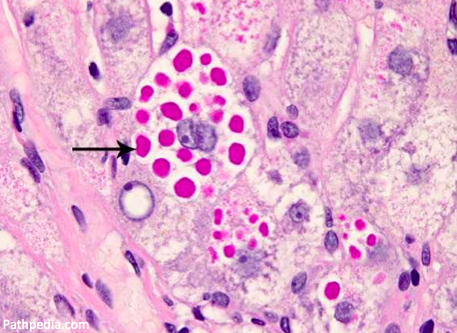
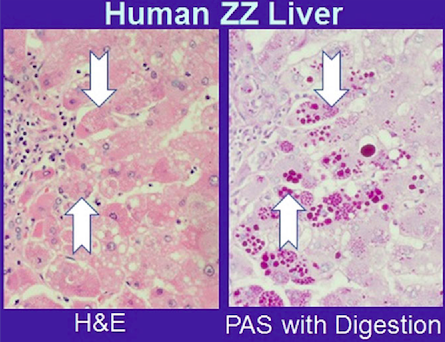
Polymerized AAT clumps together in hepatocytes, leading to histologically visible, PAS-positive inclusions.
⚡️This accumulation is called a "toxic gain of function", as opposed to the toxic loss of function that leads to emphysema.
pubmed.ncbi.nlm.nih.gov/28752441/
Polymerized AAT clumps together in hepatocytes, leading to histologically visible, PAS-positive inclusions.
⚡️This accumulation is called a "toxic gain of function", as opposed to the toxic loss of function that leads to emphysema.
pubmed.ncbi.nlm.nih.gov/28752441/
7/
A follow-up question: how do these clumps of AATs actually lead to hepatic injury?
The exact causes are not known but the leading theory involves mitochondrial damage...
A follow-up question: how do these clumps of AATs actually lead to hepatic injury?
The exact causes are not known but the leading theory involves mitochondrial damage...
8/
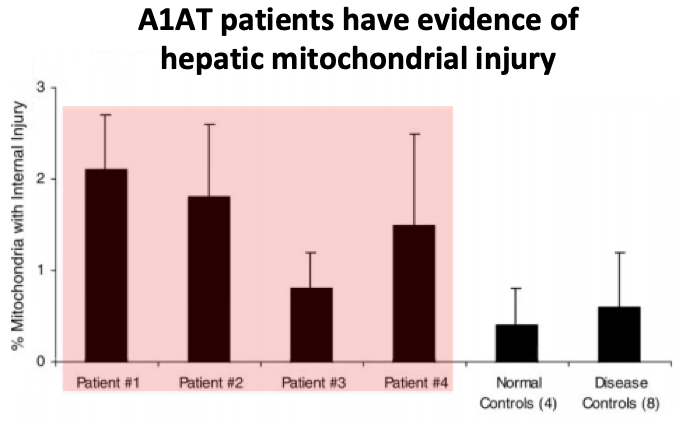
Mouse A1AT models and human patient studies have shown that clumps of AAT in the ER injure hepatic mitochondria, in a process called proteotoxic stress.
The injured mitochondria release reactive oxygen species, contributing to hepatocyte damage.
pubmed.ncbi.nlm.nih.gov/14684378/
Mouse A1AT models and human patient studies have shown that clumps of AAT in the ER injure hepatic mitochondria, in a process called proteotoxic stress.
The injured mitochondria release reactive oxygen species, contributing to hepatocyte damage.
pubmed.ncbi.nlm.nih.gov/14684378/
9/
A "null" genotype, where no circulating AAT is produced at all, get severe emphysema (b/c they make no AAT). But liver disease has never been observed.
This reinforces that the key event for liver disease development is hepatocyte AAT accumulation.
pubmed.ncbi.nlm.nih.gov/2254451/
A "null" genotype, where no circulating AAT is produced at all, get severe emphysema (b/c they make no AAT). But liver disease has never been observed.
This reinforces that the key event for liver disease development is hepatocyte AAT accumulation.
pubmed.ncbi.nlm.nih.gov/2254451/
10/
The mechanism of liver disease in A1AT has therapeutic implications as well.
For patients with severe deficiencies of AAT and emphysema, pooled donor plasma w/ AAT is often used therapeutically to replace the enzyme they don't produce.
pubmed.ncbi.nlm.nih.gov/22536580/
The mechanism of liver disease in A1AT has therapeutic implications as well.
For patients with severe deficiencies of AAT and emphysema, pooled donor plasma w/ AAT is often used therapeutically to replace the enzyme they don't produce.
pubmed.ncbi.nlm.nih.gov/22536580/
11/
💥 But because liver disease results from intra-hepatocyte inclusions of AAT, not protease deficiency, enzyme replacement has no role.
💥 But because liver disease results from intra-hepatocyte inclusions of AAT, not protease deficiency, enzyme replacement has no role.
12/
Let's end w/ an interesting association:
A1AT liver disease and obesity appear to be linked.
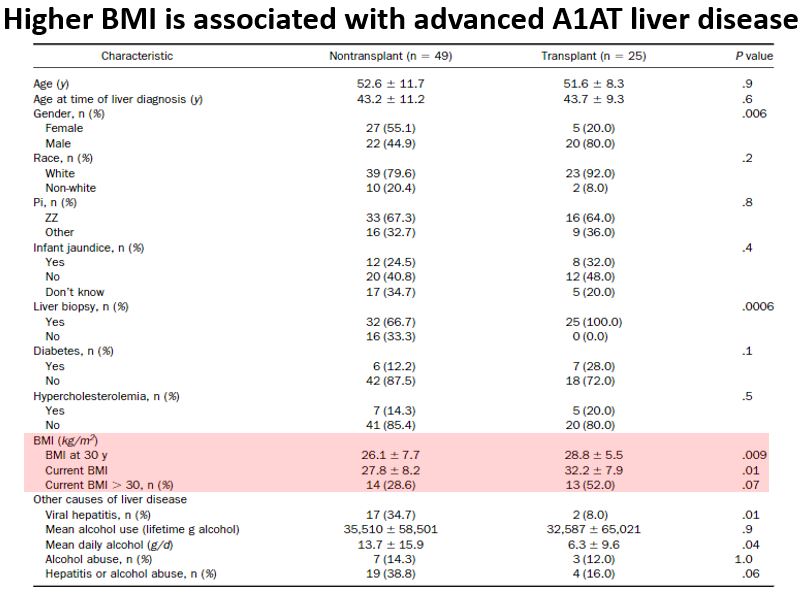
For one, obesity is a primary risk factor for progression of A1AT liver disease to cirrhosis.
pubmed.ncbi.nlm.nih.gov/15822045/
Let's end w/ an interesting association:
A1AT liver disease and obesity appear to be linked.
For one, obesity is a primary risk factor for progression of A1AT liver disease to cirrhosis.
pubmed.ncbi.nlm.nih.gov/15822045/
13/
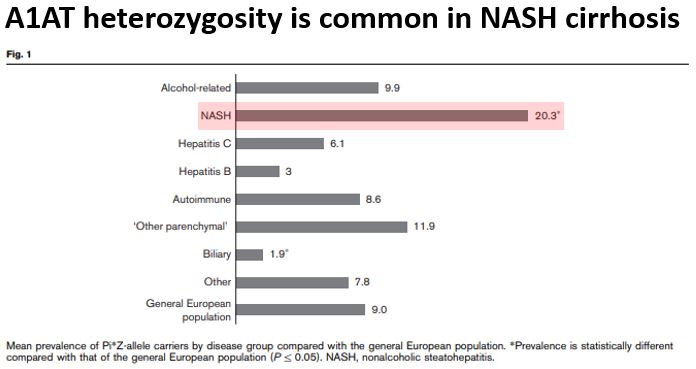
And, amazingly, heterozygosity for A1AT alleles is associated w/ progression of fatty liver disease to NASH cirrhosis.
In one study, 20% of patients w/ NASH cirrhosis had one Z mutation (much higher than would be expected in the general population).
pubmed.ncbi.nlm.nih.gov/31597010/
And, amazingly, heterozygosity for A1AT alleles is associated w/ progression of fatty liver disease to NASH cirrhosis.
In one study, 20% of patients w/ NASH cirrhosis had one Z mutation (much higher than would be expected in the general population).
pubmed.ncbi.nlm.nih.gov/31597010/
14/
Why would heterozygosity for the Z AAT allele worsen NASH?
Z heterozygotes do make some abnormal AAT. It may be that inflammatory injury from NASH interferes w/ removal of abnormal AAT (autophagy), exacerbating the underlying fatty liver disease.
pubmed.ncbi.nlm.nih.gov/31597010/
Why would heterozygosity for the Z AAT allele worsen NASH?
Z heterozygotes do make some abnormal AAT. It may be that inflammatory injury from NASH interferes w/ removal of abnormal AAT (autophagy), exacerbating the underlying fatty liver disease.
pubmed.ncbi.nlm.nih.gov/31597010/
15/
💡A1AT liver dx is due to AAT misfolding and clumping in hepatocytes, injuring mitochondria
💡= "toxic gain of function"
💡Differs from "toxic loss of function" in A1AT emphysema
💡Link b/w A1AT and obesity (obesity ⬆️ A1AT liver dx, Z allele ⬆️ risk for NASH cirrhosis)
💡A1AT liver dx is due to AAT misfolding and clumping in hepatocytes, injuring mitochondria
💡= "toxic gain of function"
💡Differs from "toxic loss of function" in A1AT emphysema
💡Link b/w A1AT and obesity (obesity ⬆️ A1AT liver dx, Z allele ⬆️ risk for NASH cirrhosis)