Our conversation with Tony Fauci was highly informative, and inspirational. A summary of key points of the podcast and commentary w/ @cuttingforstone @Medscape medscape.com/viewarticle/93…
1. The #SARSCoV2 virus in unique
1. The #SARSCoV2 virus in unique
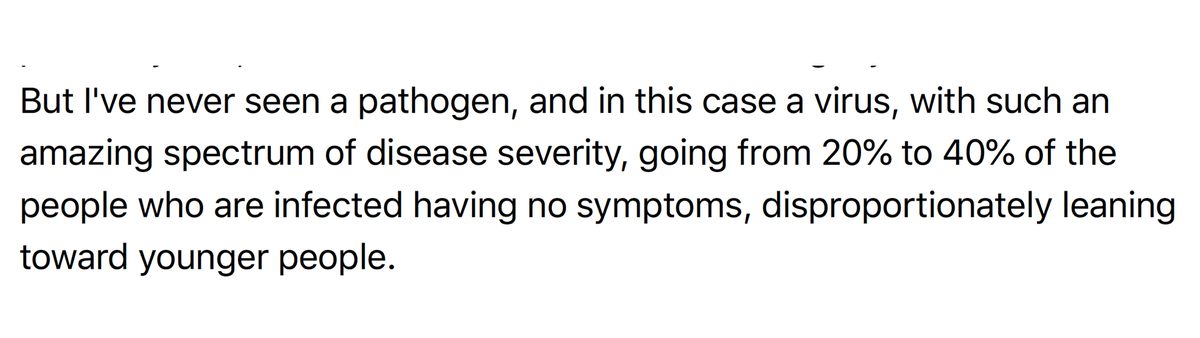
2. That's 20-40% of people who get infected and never show symptoms. More likely in young. Who don't understand they are propagating the pandemic
"Usually a virus that is good enough to kill you would make almost everybody at least a little bit sick."
"Usually a virus that is good enough to kill you would make almost everybody at least a little bit sick."
3. The chronic "long covid" post-viral symptoms of #COVID19 are common, understudied to date.
"And it's extraordinary how many people have a postviral syndrome that's very strikingly similar to myalgic encephalomyelitis/chronic fatigue syndrome."
"And it's extraordinary how many people have a postviral syndrome that's very strikingly similar to myalgic encephalomyelitis/chronic fatigue syndrome."
4. We don't have a #COVID19 czar with decision-making authority, like @RonaldKlain for Ebola (who Fauci loves) but @VP has taken on a lead role, is receptive, and "deeply involved." Fauci is very respectful to the Administration despite all the efforts of @POTUS to undermine him
5. What about the @HHSgov hijacking the @CDCgov covid data?
Fauci only learned about it by watching television
Fauci only learned about it by watching television
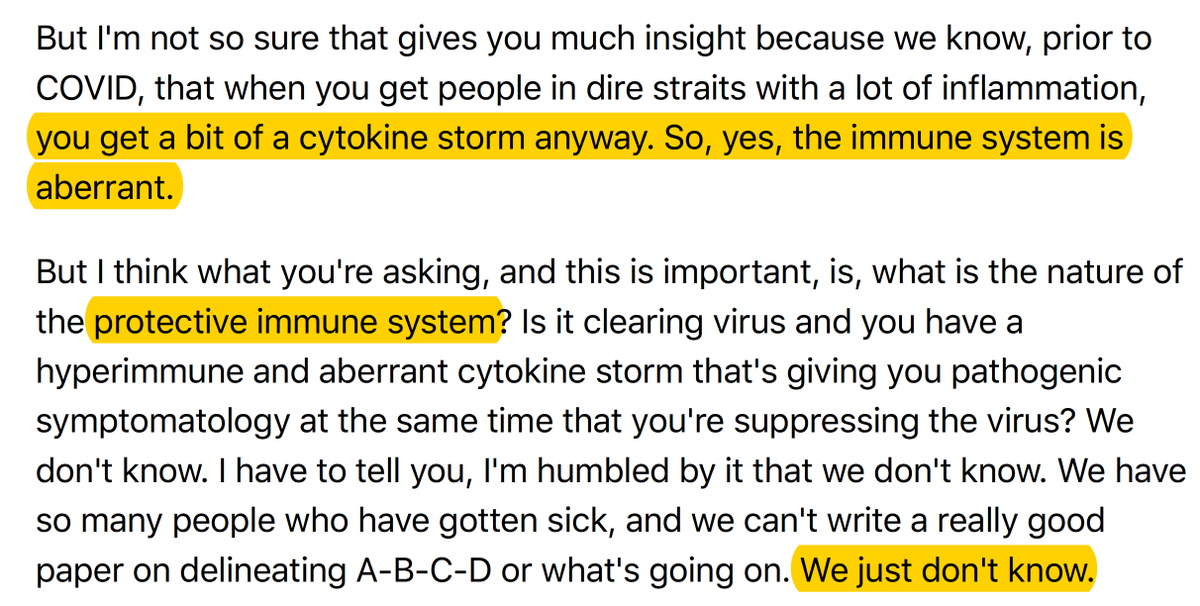
6. What about the hyperimmune response to #COVID19 and that being implicated as the basis for most fatalities?
7. It took 5 days from the sequence of #SARSCoV2 to Fauci's team to get the start on a vaccine, 62 days to get Phase 1 clinical trial started (That is simply incredible)
8. What about short-lived antibodies to the virus and the role of T cells?
#SARSCoV2 is like SARS with a significant and enduring T cell response. We shouldn't be worried about the IgG antibody waning report that got a lot of buzz this week.
#SARSCoV2 is like SARS with a significant and enduring T cell response. We shouldn't be worried about the IgG antibody waning report that got a lot of buzz this week.
9. What about reinfection, does it occur?
There are anecdotes, but no proof of replication competent virus. So if it really exists it's rare (considering millions of infections). Hard to prove since you need a BSL-3 lab to correlate PCR results of RNA nucleotides w/ live virus
There are anecdotes, but no proof of replication competent virus. So if it really exists it's rare (considering millions of infections). Hard to prove since you need a BSL-3 lab to correlate PCR results of RNA nucleotides w/ live virus
10. On the mask pushback, Fauci attributes this to the "disturbing anti-science trend" My worry is that will extend to implementing the vaccine, but we didn't get to that issue
11. Monoclonal (neutralizing) antibodies were developed for Ebola and highly successful They are now in clinical trials for SARSCoV2, very potent, and will likely be used in early and late stages of treatment. Mabs don't get the attention of vaccines but very important & imminent
12. Rapid diagnostic kits for home or point of care are in the works, NIH has invested $500 million, results in < 30 mins. These will be transformative when they are available this fall
13. Favorite part: his comments to the frontline heroes and how science will prevail.
• • •
Missing some Tweet in this thread? You can try to
force a refresh