#SARSCOV2 transmission in children vs adults
Obviously a v important topic.
New paper @mlipsitch @mugecevik @EdwardGoldste16. I have serious issues w/ conclusions because it ignores well-known biases, conflates infection & susceptibility, & misuses anecdotes.
Thread.
Obviously a v important topic.
New paper @mlipsitch @mugecevik @EdwardGoldste16. I have serious issues w/ conclusions because it ignores well-known biases, conflates infection & susceptibility, & misuses anecdotes.
Thread.
Background
A huge Q about transmission of SARS-COV-2 is how transmission varies by age. Specifically, is there age-specific variation in either susceptibility or infectiousness?
Many ways to address this Q, but most have major challenges due to biases in how data are collected.
A huge Q about transmission of SARS-COV-2 is how transmission varies by age. Specifically, is there age-specific variation in either susceptibility or infectiousness?
Many ways to address this Q, but most have major challenges due to biases in how data are collected.
What we DO know is that disease severity shows huge age variation.
See end of thread for age-specific fatality estimates:
Also paper by @hsalje shows age-specific hospitalization which shows similar huge skew towards older people.
10.1126/science.abc3517
See end of thread for age-specific fatality estimates:
Also paper by @hsalje shows age-specific hospitalization which shows similar huge skew towards older people.
10.1126/science.abc3517
This suggests probability of asymptomatic (or mildly symptomatic) infection will be higher for young people. I haven't seen direct data on this Q & again challenging to collect b/c of possibility of missing asymptomatic infection & bias in recall of symptoms if using serology.
Why does this matter? Because detection of both index cases and secondary cases often depends on detecting symptoms. Since we know that severe symptoms increase w/ age we know there will be strong bias against seeing young as primary cases.
In addition, if contacts of young index cases are also young (age-specific mixing, especially when schools are open), then we expect to miss many infections because of a lower prob of symptoms.
A lower prob of symptoms also biases studies of infection. If child is index case but shows no symptoms & infects parent who shows symptoms later & you then test child, chance you miss infection is quite high. @c_drosten & I both note this:
In addition, infection is product of contact rate & susceptibility. A lower infection rate (if one could correct for biases) implies EITHER lower susceptibility or lower contact rate. I've had many discussions w/ families & ALL report attempting to shield children from infection.
This meant sequestering in a room when sick, only interacting with other parent, etc.
Who did parents try to shield the most? Their youngest children.
Who did parents try to shield the most? Their youngest children.
I'd make 2 strong assertions:
-One should not make any claims about relative susceptibility based on infection data; relative contact rates (shielding) equally (more?) likely.
-Claims about relative infection patterns are suspect because of biases due to differential symptoms
-One should not make any claims about relative susceptibility based on infection data; relative contact rates (shielding) equally (more?) likely.
-Claims about relative infection patterns are suspect because of biases due to differential symptoms
Can other data help? Yes!
Seroprevalence studies remove one of these issues (but not the other) - differential prob of symptoms
Paper discusses serological data but strangely doesn't make figure or table. Text barely mentions children vs adults.
Seroprevalence studies remove one of these issues (but not the other) - differential prob of symptoms
Paper discusses serological data but strangely doesn't make figure or table. Text barely mentions children vs adults.
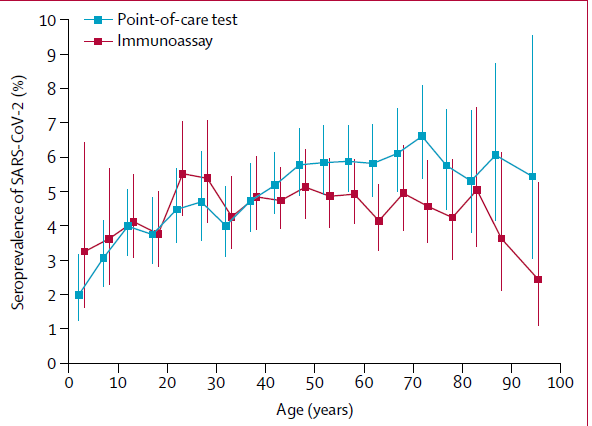
I'd like to see authors assemble all the data and show it visually. My read of papers they discuss is that evidence is mixed. Some papers show lower seroprevalence in children (fig), some don't. But remember that most data come from periods when schools were closed. 
Thus, children's normal contact rates are not occurring. This means that lower exposure/infection measured by serology could mean lower contact rates OR lower susceptibility.
In case it wasn't obvious why this matters, here's why:
If lower exposure was due to lower contact rates and not lower susceptibility, then when we re-open schools transmission would be high unless protective measures are taken.
If lower exposure was due to lower contact rates and not lower susceptibility, then when we re-open schools transmission would be high unless protective measures are taken.
Finally, several papers already attempted to assess age-specific susc./infection & weren't cited or discussed. In general, paper was missing many hugely important papers. Two obvious ones:
medrxiv.org/content/10.110…
nature.com/articles/s4159…
medrxiv.org/content/10.110…
nature.com/articles/s4159…
In case some of this sounds familiar, yes, I've written about this before:
What about infectiousness? Not many papers & again many challenges in interpreting data b/c hard to know direction of infection - who infected who?
An ongoing challenge is that contact tracing studies define person w/ earlier symptom onset as index case & later as infectee.
An ongoing challenge is that contact tracing studies define person w/ earlier symptom onset as index case & later as infectee.
This clearly biases against IDing children as index cases b/c less symptomatic. Also, if child is index case who infects sibling, who infects parent then even if 2nd child is ID'd as index case, testing 1st child will likely miss infection & bias attack rate from children lower.
Biggest dataset on relative infectivity by age is recent S Korea study. I've written about what we can and can't conclude from that study in detail here:
How can these issues be addressed? Combining qPCR & serological assays w/in households won't miss older infections & will better define transmission chains. This study is a great example that should be done more:
thelancet.com/action/showPdf…
thelancet.com/action/showPdf…
Other major way to examine infectivity (besides fraction of contacts infected) is viral loads when infected. New paper discusses one study on this but misses another big one.
medrxiv.org/content/10.110…
I wrote about it here:
medrxiv.org/content/10.110…
I wrote about it here:
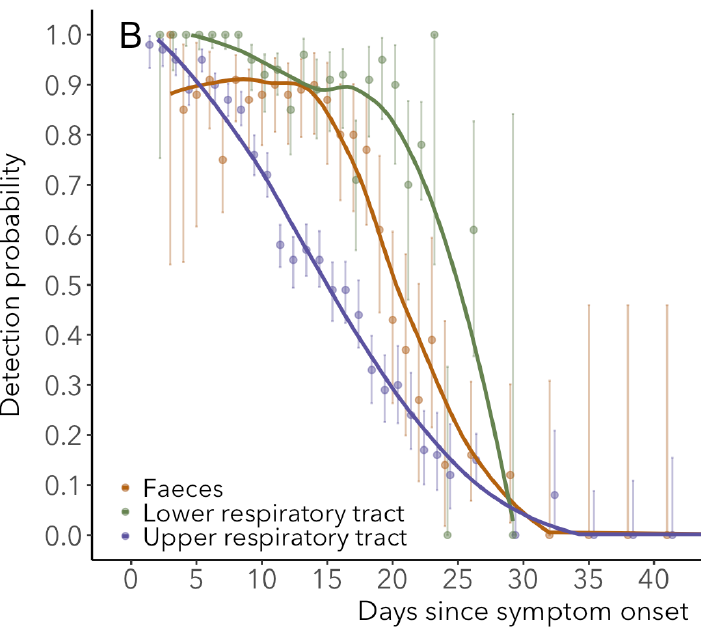
Data on viral loads indicate no difference among children & adults but even these data are hard to collect in unbiased way, again due to lower prob symptoms of kids. Read details of challenges in paper by @c_drosten
medrxiv.org/content/10.110…
medrxiv.org/content/10.110…


Finally, paper discusses recent school re-openings as anecdotal evidence for what happens when schools are open since most early studies were when schools were closed. I found discussion biased, & used to try to support earlier conclusions rather than balanced assessment.
There are unfortunately now many examples of substantial transmission w/in schools (check out @DrZoeHyde posts & follow her). Most are just press reports so hard to know who infected who, but to me they clearly indicate plenty of transmission into & within school.
Conclusion:
Data do not support strong claim of lower susceptibility in children.
I'd argue we CANNOT make any claims about susceptibility b/c we can't separate susceptibility from contact.
I'd even caution against making claims about infection b/c biases & schools closed.(cont)
Data do not support strong claim of lower susceptibility in children.
I'd argue we CANNOT make any claims about susceptibility b/c we can't separate susceptibility from contact.
I'd even caution against making claims about infection b/c biases & schools closed.(cont)
What can we say? I think the data irrefutably indicate that children CAN be infected & often at similar levels (serology) & schools will increase this further.
I think data also indicate irrefutably that kids can transmit the virus to each other & adults. I don't think rigorous studies exist to determine if they do so 1/2 as much or 3/4 or equally & I don't think it matters.
Regardless of which is correct, I think all epidemiologists would still recommend the same course of action to re-open schools safely: We need to reduce community transmission & put measures in place to reduce risk in schools - masks, distance, ventilation, cohorting, etc.
Quick addition. Just learned of this paper by the always sharp @jLewnard et al that addresses this and other questions w/ data from India. Haven't had a chance to read it yet but it shows different patterns & I'd like to know why. More later.
medrxiv.org/content/10.110…
medrxiv.org/content/10.110…

Addition: @DrZoeHyde put together another thread today with many links to recent outbreaks in children as well as discussion of key issues: