Dear Nobel Prize Committee,
I would like to claim my Nobel Prize please.
For curing cancer.
Can you post me my medal, or do I have to come and collect it in person?
#FOAMED #MedTwitter #Tweetorial
I would like to claim my Nobel Prize please.
For curing cancer.
Can you post me my medal, or do I have to come and collect it in person?
#FOAMED #MedTwitter #Tweetorial
Thank you to @RicardoPetraco and @mshunshin for drawing this to my attention, but I will have the Nobel on my own thanks, as I am the boss. You guys are basically just Rosalind Franklin.
The method of curing cancer I have developed is as follows.
The method of curing cancer I have developed is as follows.
You know the BP pills that you are mostly taking?
Well, take them at night.
That's it.
Well, take them at night.
That's it.
Here is my reasoning.
You know this paper, that patients keep bringing and asking about?
You know this paper, that patients keep bringing and asking about?
Source: academic.oup.com/eurheartj/arti…
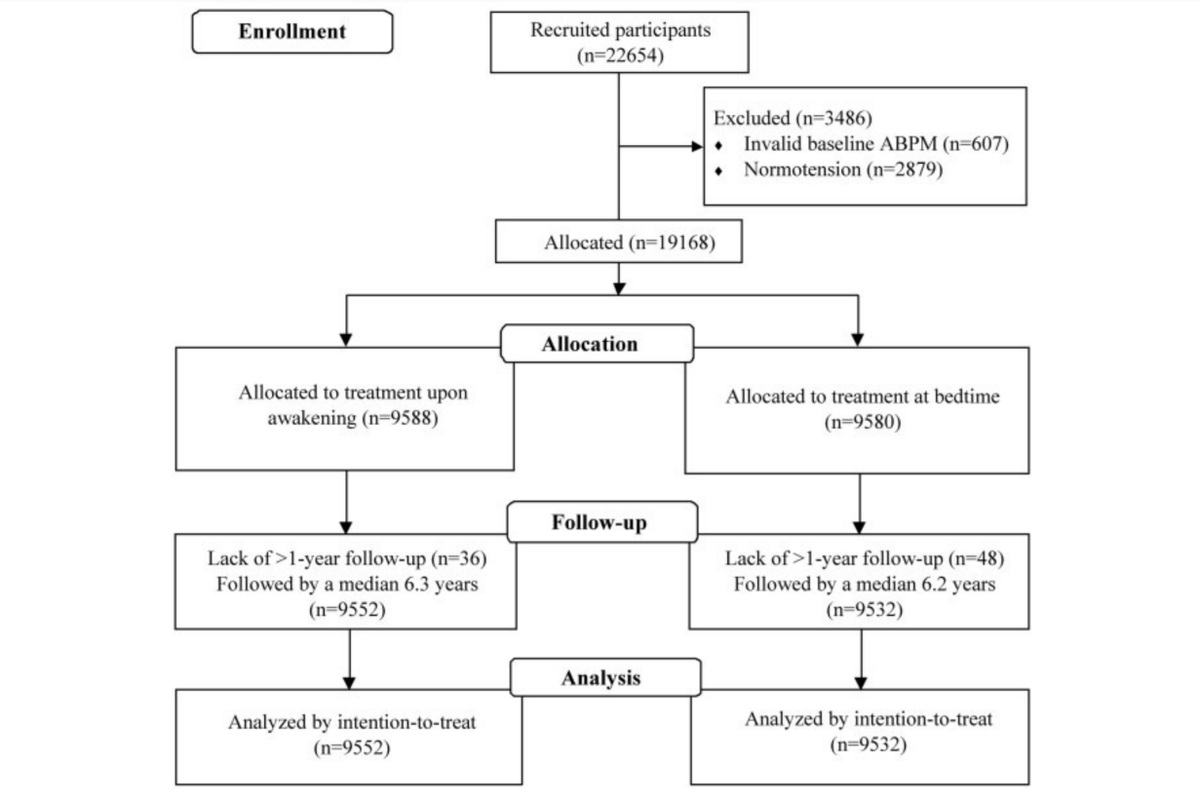
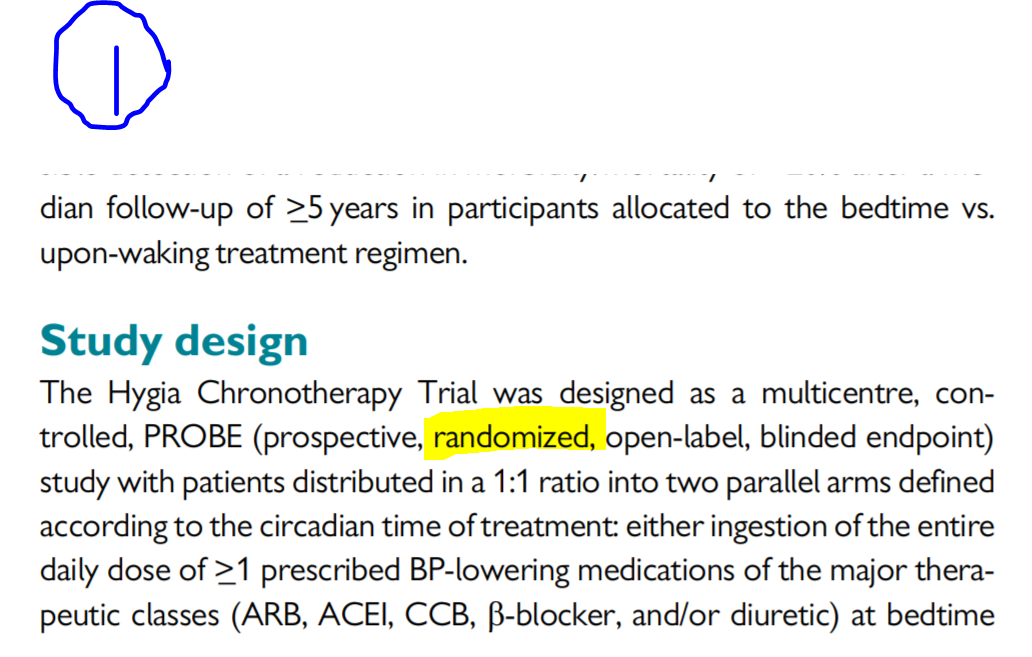
Remember the paper? The one with the strange feature whereby they couldn't bring themselves to write the word "randomized" in the flow chart?
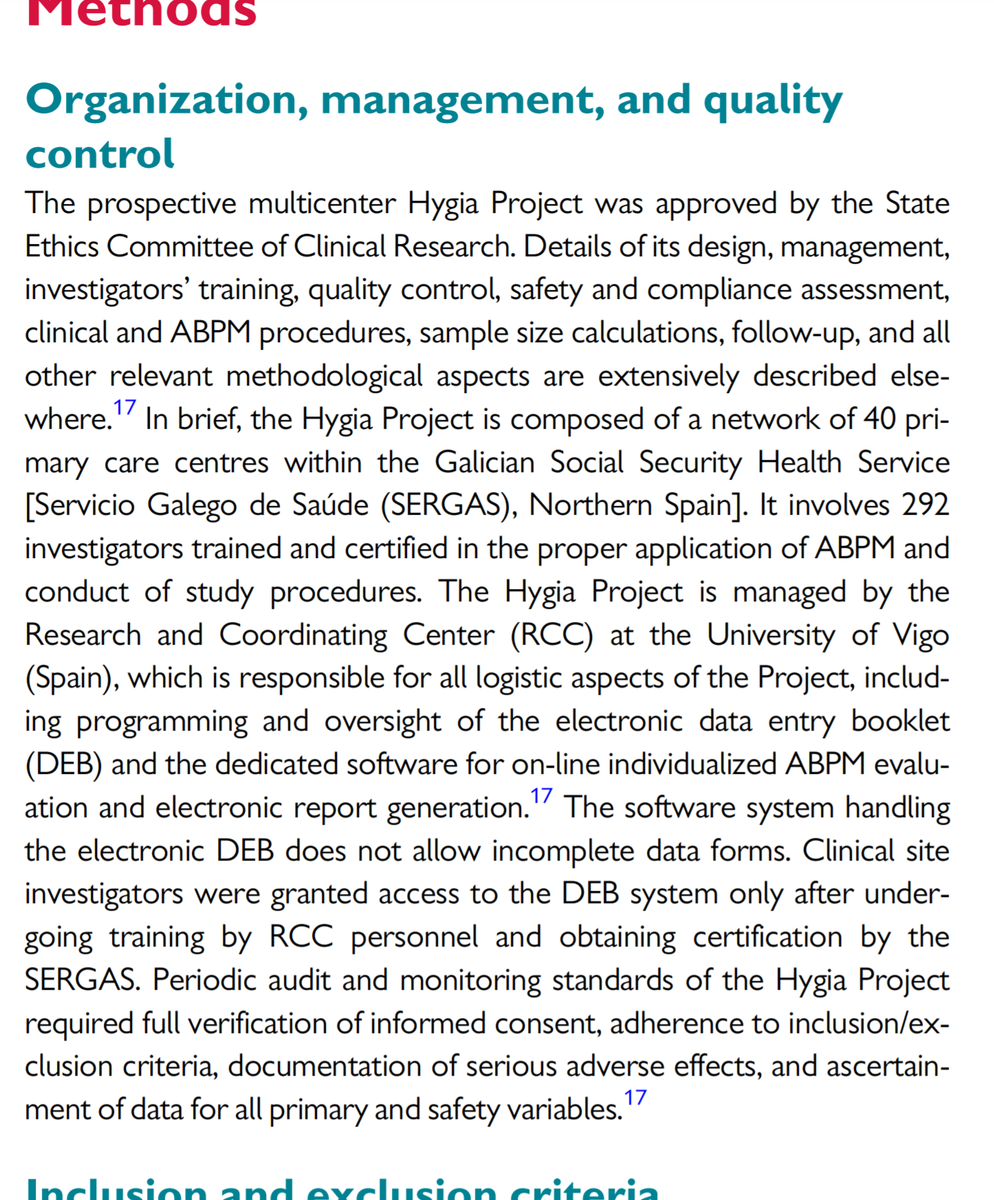
The description of the randomization process is given here.
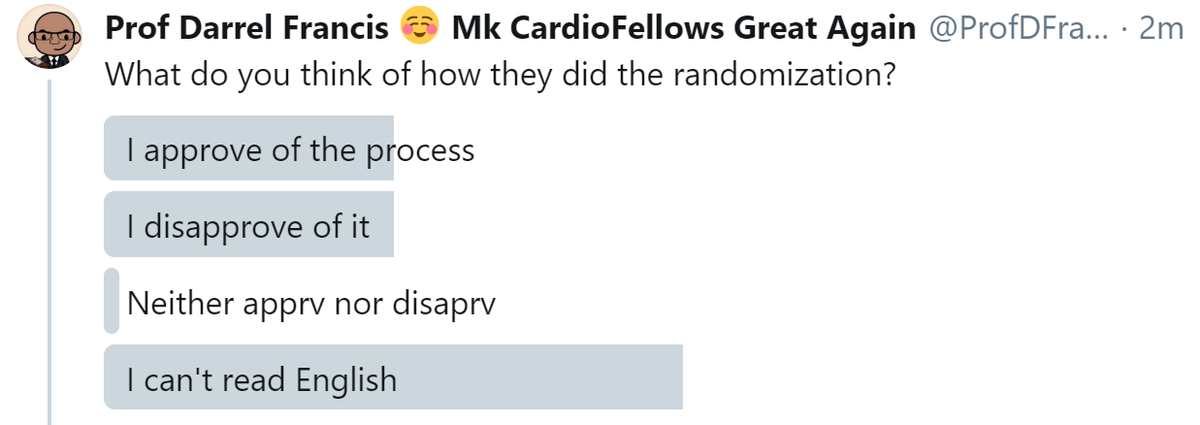
What do you think of how they did the randomization?
The only acceptable answer is C.
(Or maybe D, I suppose, if you used Google Translate to do the poll.)
(Or maybe D, I suppose, if you used Google Translate to do the poll.)
Because here is what it said about the randomization method:

Oh dear.
It is human nature to avoid lying. As a magistrate in British-ruled India once said to a witness who was obviously being untruthful,
"Don't tell unnecessary lies."
"Don't tell unnecessary lies."
The interpreter conveyed this into Hindi, but unfortunately conveyed a different subtley:
"Judge Sahib says, you must tell lies only when it is necessary".
"Judge Sahib says, you must tell lies only when it is necessary".
Anyway that stuff won't get me my Nobel.
Let's do some serious numbers.
Let's do some serious numbers.
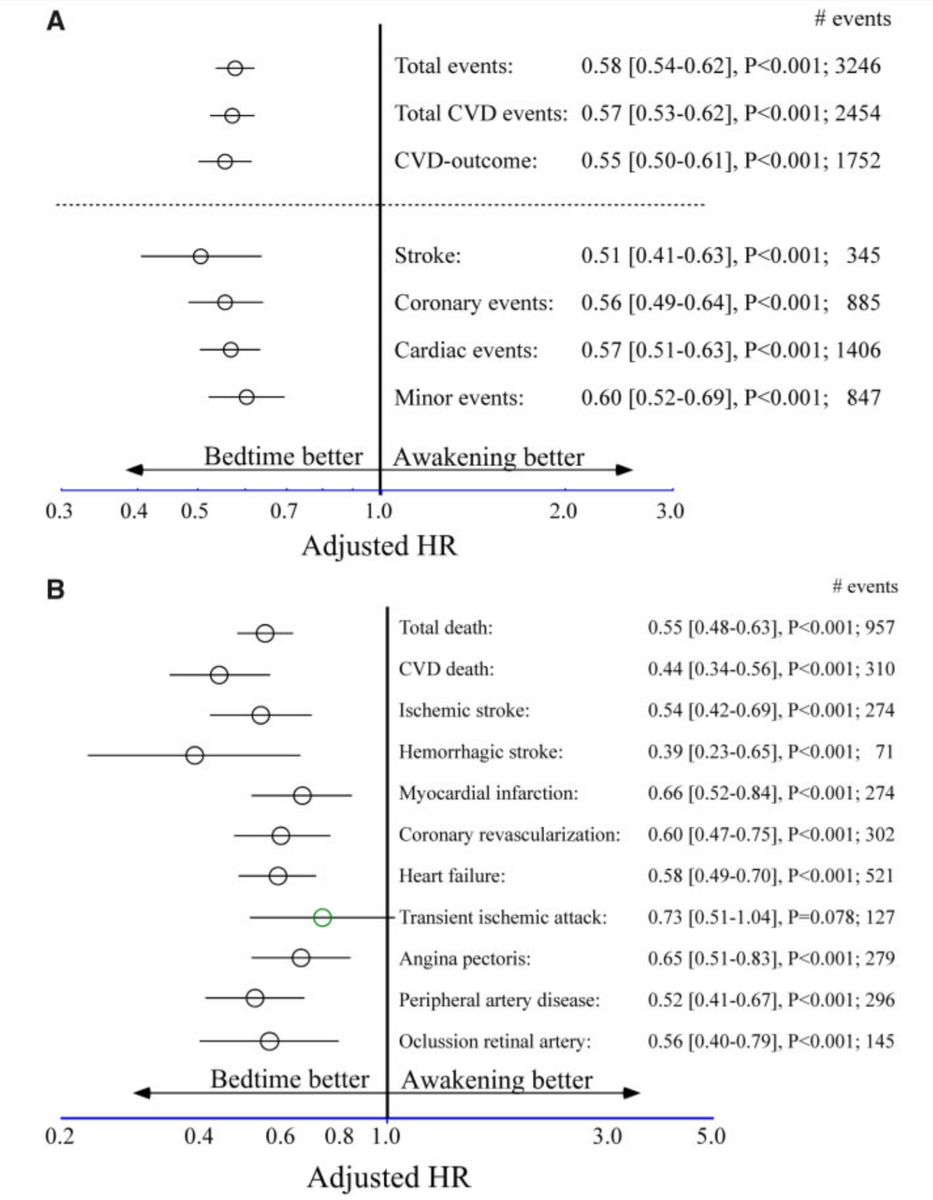
Looks good, eh?
How many died in total?
How many died in total?
Right, well 2 out of the first 3 people have managed to read three digits correctly, so I am feeling uncharacteristically optimistic about today.
HAZARD ratio for all-cause mortality was 0.55.
[Since only a small proportion of the participants died, and followup was pretty complete...]
Which of the following is your best estimate for the RISK ratio for mortality. Also called relative risk or probability ratio.
[Since only a small proportion of the participants died, and followup was pretty complete...]
Which of the following is your best estimate for the RISK ratio for mortality. Also called relative risk or probability ratio.
Yes. Remember that "hazard" is just a way of preventing probabilities getting crushed up near 1 when probability of death is high.
For example, imagine I go driving my car at 100 miles an hour at 2 times the alcohol limit, for an hour. The chances of dying might be (say) 90%.
Then I say, how about driving for 2 hours like that instead?
Probability of death may be 99%. But this is only 9 percentage points higher.
Probability of death may be 99%. But this is only 9 percentage points higher.
"What is the relative risk of driving a two hour journey versus a one hour journey, in both cases at 100 miles per hour and at double the alcohol limit?"
Suppose the mortalities are 90 and 99% respectively.
Suppose the mortalities are 90 and 99% respectively.
Well, I may have planned to drive in a heavily inebriated state to @LCC_DrMalik's house to call him a big fat pillock, but I may as well go the whole hog and drive to NHS England and shout at the people who say coughing isn't an Aerosol Generating Procedure.
RR is only 1.1.
RR is only 1.1.
So RR isn't a good marker when risk gets close to 1. That is because, basically, when you're dead, you're dead.
Being very dangerous (in risk, aka probability terms) prevents anything being more dangerous in comparison.
Being very dangerous (in risk, aka probability terms) prevents anything being more dangerous in comparison.
Hence the invention of Hazard. It is a version of risk (probability) that DOES NOT STOP AT 1.
What they do is like how glass blowers make glass.
What they do is like how glass blowers make glass.

In short, they take the bit near "probability 1" and stretch it out above 1. So things can be more dangerous than 1.
Obviously they can't just do it for big probabilities, and leave small probabilities alone. That would create a discontinuity.
They have to smoothly stretch.
Obviously they can't just do it for big probabilities, and leave small probabilities alone. That would create a discontinuity.
They have to smoothly stretch.
They would want to do MINIMAL stretching near p=0, and MAXIMAL stretching near p=1.
So low probabilities get let through unchanged, like this:
So low probabilities get let through unchanged, like this:
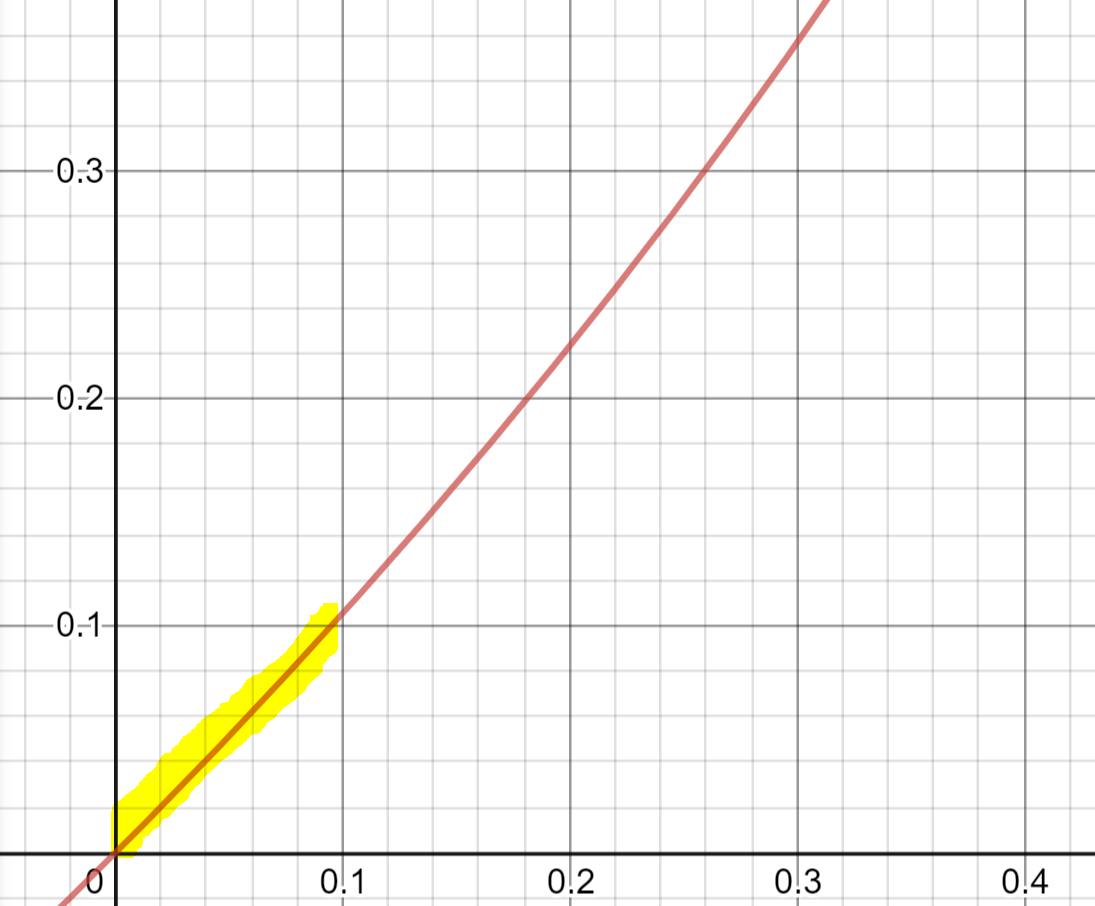
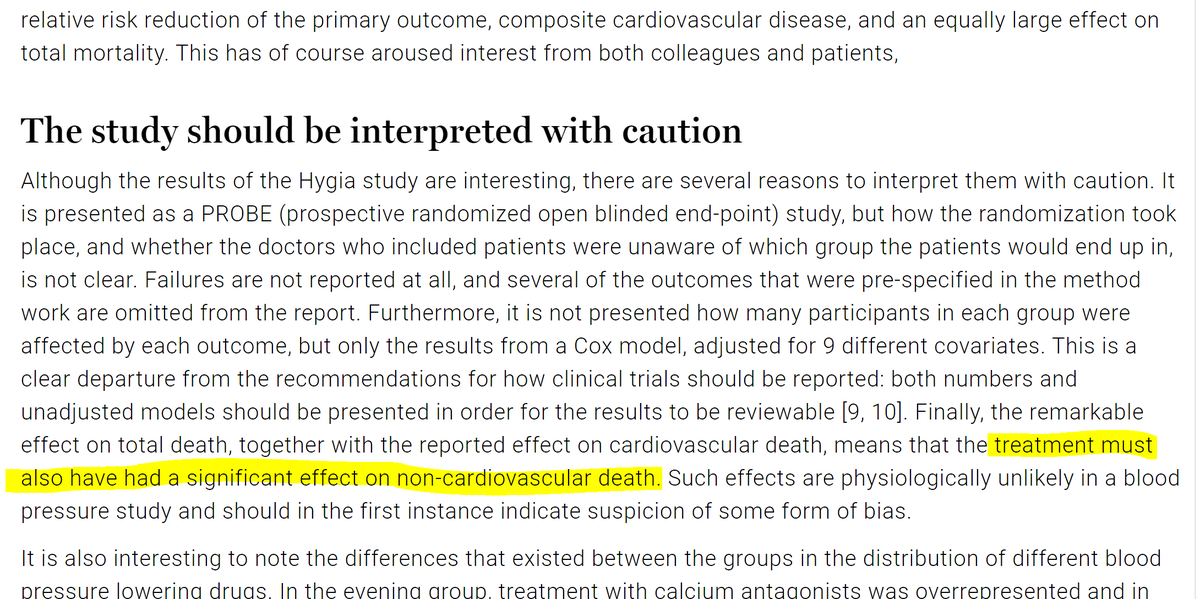
But when the probability gets close to 1, the curve goes up and up, faster and faster.
In this figure, blue dashes show what the original probability looks like, and the red curve is the upward-bent alternative we want.
In this figure, blue dashes show what the original probability looks like, and the red curve is the upward-bent alternative we want.

In short, we want something that looks like this.
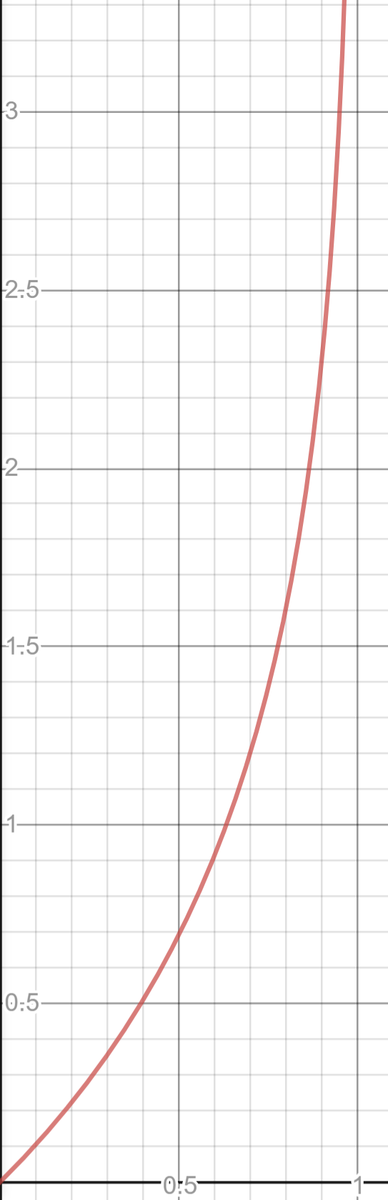
Happily, there exists a lovely function in Maths, that will do this for us. It is an exponential curve, but reversed, so it is a logarithm.
y = - ln(1-x)
y = - ln(1-x)
It has nice properties.
By the chain rule,
dy/dx
= -1 * 1/(1-x) * d/dx(1-x)
= 1/(1-x)
By the chain rule,
dy/dx
= -1 * 1/(1-x) * d/dx(1-x)
= 1/(1-x)
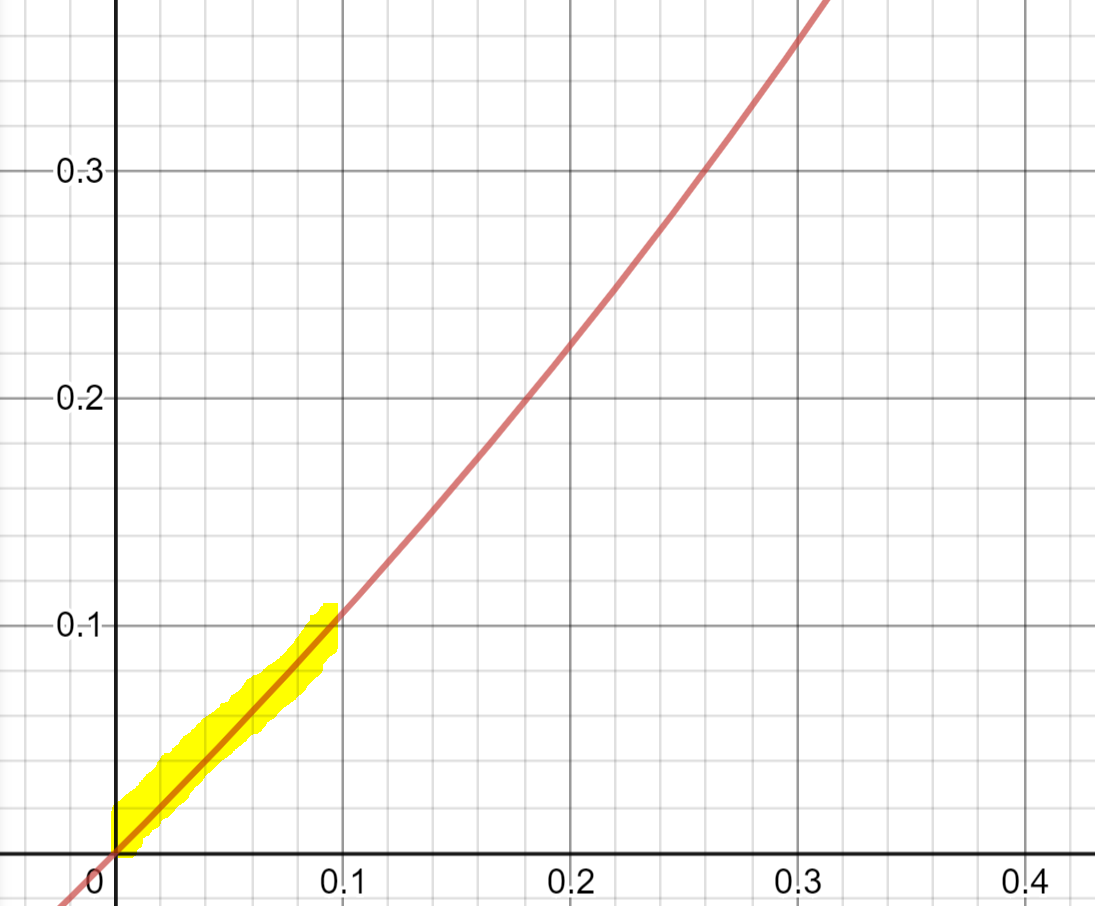
This means at x=0, the slope is 1/(1-0)=1, i.e.
For low probabilities,
hazard is almost exactly the same as probability.
And as probability increases, the curve gets steeper in proportion to 1/(1-probability).
For low probabilities,
hazard is almost exactly the same as probability.
And as probability increases, the curve gets steeper in proportion to 1/(1-probability).
Now let's check our drink-drive travel plans on a proper scientific basis.
90% chance of death is what HAZARD of death?
- ln(1-0.9) is what?
Hint: lmgtfy.com/?q=-ln(1-0.9)
90% chance of death is what HAZARD of death?
- ln(1-0.9) is what?
Hint: lmgtfy.com/?q=-ln(1-0.9)
Answer?
And how about the longer journey?
Shouting abuse at Iqbal Malik and then vomiting at NHS England, saying "How about that for an aerosol?"
Convert 0.99 probability to a HAZARD.
- ln (1-0.99) is what?
Hint: google.com/search?q=-ln(1…
Shouting abuse at Iqbal Malik and then vomiting at NHS England, saying "How about that for an aerosol?"
Convert 0.99 probability to a HAZARD.
- ln (1-0.99) is what?
Hint: google.com/search?q=-ln(1…
Answer:
So the hazard RATIO, for the more dangerous in relation to the less dangerous, is what?
Strange that it is so exact, eh?

Not really.
It is exact because that is exactly what hazards do.
They allow linear combinations of dangerous things, like a 100 mile journey and then another identical journey, to add up linearly, rather than get squashed up at 1.
It is exact because that is exactly what hazards do.
They allow linear combinations of dangerous things, like a 100 mile journey and then another identical journey, to add up linearly, rather than get squashed up at 1.
Anyway, back to my Nobel prize.
That's the main point of today!
About 20k patients and 1k deaths.
Probability of death was therefore (choose the option that best describes the answer):
That's the main point of today!
About 20k patients and 1k deaths.
Probability of death was therefore (choose the option that best describes the answer):
So will probabilities and hazards, given what you have seen on the graph of -ln(1-x) above, be:
For some reason the first two people chose option A. This is disappointing.
At probabilities around 1/20th, i.e. 0.05, hazards are very similar to probabilities, so we can just treat the hazard ratio as though it was a probability.
At probabilities around 1/20th, i.e. 0.05, hazards are very similar to probabilities, so we can just treat the hazard ratio as though it was a probability.
It is in fact for impatient people that I try to put some edu into the edutainment. 8-)

So we have concluded that we can say that ROUGHLY SPEAKING the ratio of probabilities of deaths is 0.55 between the two arms.
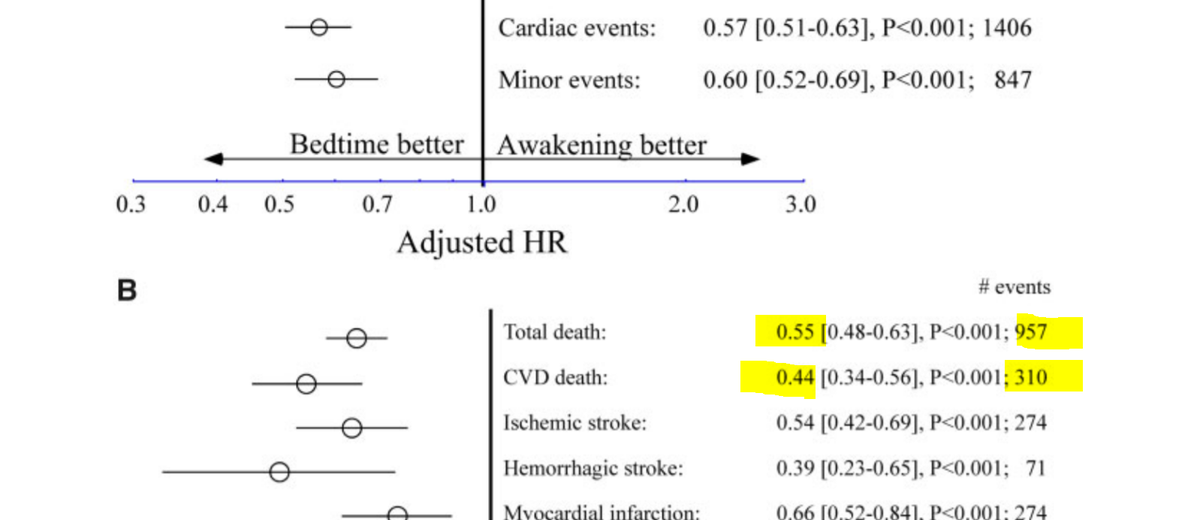
So the deaths will be apportioned between the arms in ratio approximately 0.55:1.
So the numbers of deaths in each arms will be approximately
957 *0.55/1.55 and 957 * 1/1.55 respectively,
i.e.
340 and 617.
So the numbers of deaths in each arms will be approximately
957 *0.55/1.55 and 957 * 1/1.55 respectively,
i.e.
340 and 617.
Now you try the CV deaths.
How many in the active arm?
How many in the active arm?
And the remainder of the 310 CV deaths are in the control arm, which means how many?
Here is the Nobel-prize winning discovery.
How many non-cardiovascular deaths in each arm?
245 in the active, and 402 in the control!
What's the hazard ratio, roughly?
How many non-cardiovascular deaths in each arm?
245 in the active, and 402 in the control!
What's the hazard ratio, roughly?
I am brushing up on my Swedish so I can give some fake-modest remarks on the podium.
If this 'trial' is real, I am the Queen of Denmark.
What a hilarious thing to see in a journal.
I absolutely love it.
What a hilarious thing to see in a journal.
I absolutely love it.
I can think of two possibilities.
Hypothesis 1. It wasn't really randomized. They just said it was.
My reasoning for this is that they tried really hard to avoid mentioning randomization.
Hypothesis 1. It wasn't really randomized. They just said it was.
My reasoning for this is that they tried really hard to avoid mentioning randomization.
Search the paper for the string "rand" and you see it only 3 times.

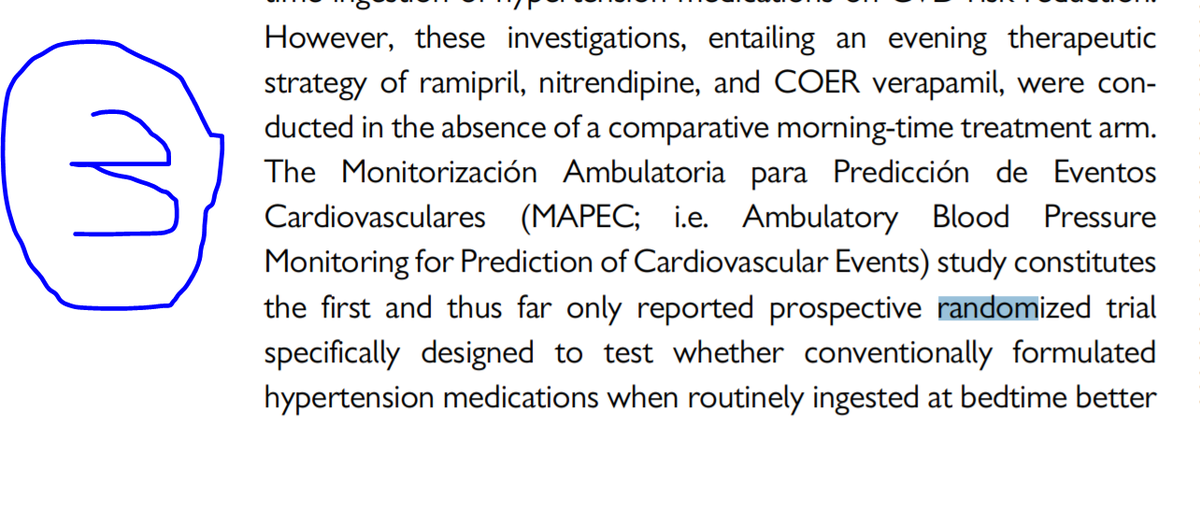
Of the three cases above, how many of the mentions of the word "randomized" referred to the HYGIA trial itself (rather than other trials?
And on the first of those occasions, what was the reason for mentioning the word "randomized"?
I don't recall ever seeing a paper about an RCT which had the character sequence "randomi" solely in reference to explaining an abbreviation, talking about OTHER trials, or reference lists.
So I think these are fundamentally honest people who wanted to lie as little as possible.
Hypothesis 2.
Actually I've forgotten what my alternative hypothesis was. I am sure I had another explanation, but was
Actually I've forgotten what my alternative hypothesis was. I am sure I had another explanation, but was
I'm sure the trial will be retracted in due course, and we should be gracious with the authors. I'm sure they meant well.
The easier we allow them to suddenly remember that it wasn't randomized, the easier it will be for them to get out of it, and the best for everyone.
The easier we allow them to suddenly remember that it wasn't randomized, the easier it will be for them to get out of it, and the best for everyone.
Men om det inte dras tillbaka är jag fortfarande tillgänglig för Nobeln.
Oh dear, what a shame.
We've noticed that quite a bit. People come out with a study where injection of the word "randomized" casues an enormous amount of unquestioning acclaim, and they then can't help themselves from getting deeper into it.
We are pressing the Lancet to retract another paper which has the same theme: implausible effect in an "RCT" followed up by more substudy reports, further entrapping the poor authors.
Haven't heard back from Lancet for a couple of years on that one. Must prod them.
Haven't heard back from Lancet for a couple of years on that one. Must prod them.
Nope.
Suggests to me that it either wasn't an RCT at all.
Or was simply made up in its entirety.
Suggests to me that it either wasn't an RCT at all.
Or was simply made up in its entirety.
Damn and blast!
Swapnil Hiremath beat me to the Nobel!
Gaaah!
Swapnil Hiremath beat me to the Nobel!
Gaaah!
Woah. If I click any of the links in Sawpnil's thread, EVEN PUBMED ITSELF joins in the laughter.
Sorry Swapnil, Nobel prize for fiction goes to not you, nor me, nor even Pubmed's cheeky web server, but to a certain R C Hermida!
He is a master japester. 8-)
Sorry Swapnil, Nobel prize for fiction goes to not you, nor me, nor even Pubmed's cheeky web server, but to a certain R C Hermida!
He is a master japester. 8-)

So when he was referencing those 'other' trials, they were his own!
This is superb!
Can anyone suggest to me which serial fibber @drgrahamcole and I are hassling the Lancet over?
Strangely similar modus operandi.
This is superb!
Can anyone suggest to me which serial fibber @drgrahamcole and I are hassling the Lancet over?
Strangely similar modus operandi.
Thank you for this Terry Bauch!
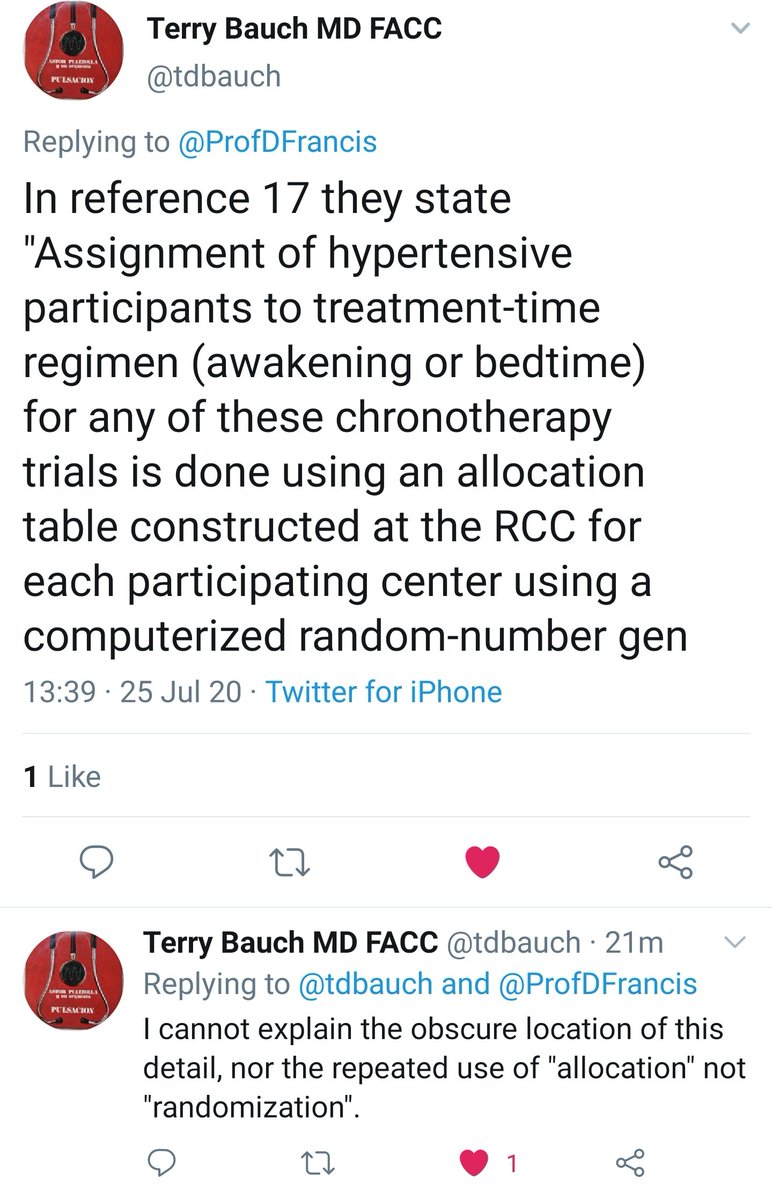
Maybe they reasoned it this way.
Suppose we outsource all the lying to one particular paper. Then we can always just reference that paper. So we avoid telling any MORE lies.
Suppose we outsource all the lying to one particular paper. Then we can always just reference that paper. So we avoid telling any MORE lies.
Dear Santa, if I never tell any more lies, will I get Christmas presents for being a good boy?
Yes?
Oh that's great !
Yes?
Oh that's great !

P.s.
It's Ok with you if I keep referencing an older off-balance-sheet lie, isn't it?
I was taught that by a friend in Wirecard.
Lovely chap.
Ok thanks.
It's Ok with you if I keep referencing an older off-balance-sheet lie, isn't it?
I was taught that by a friend in Wirecard.
Lovely chap.
Ok thanks.
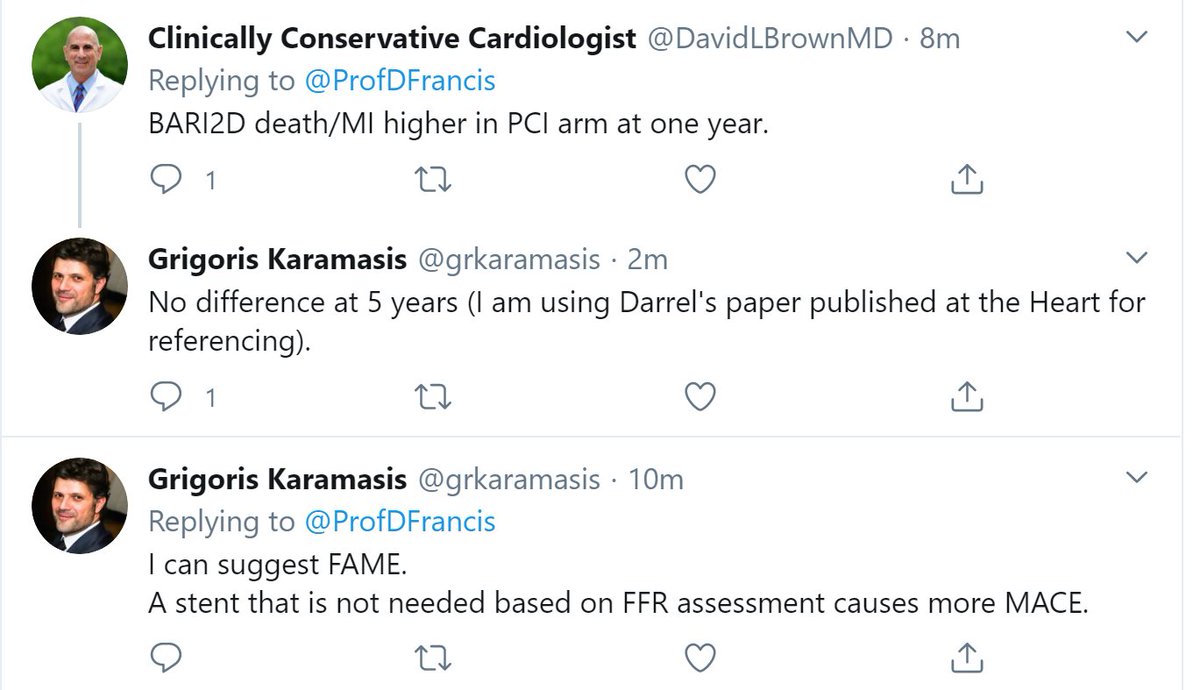
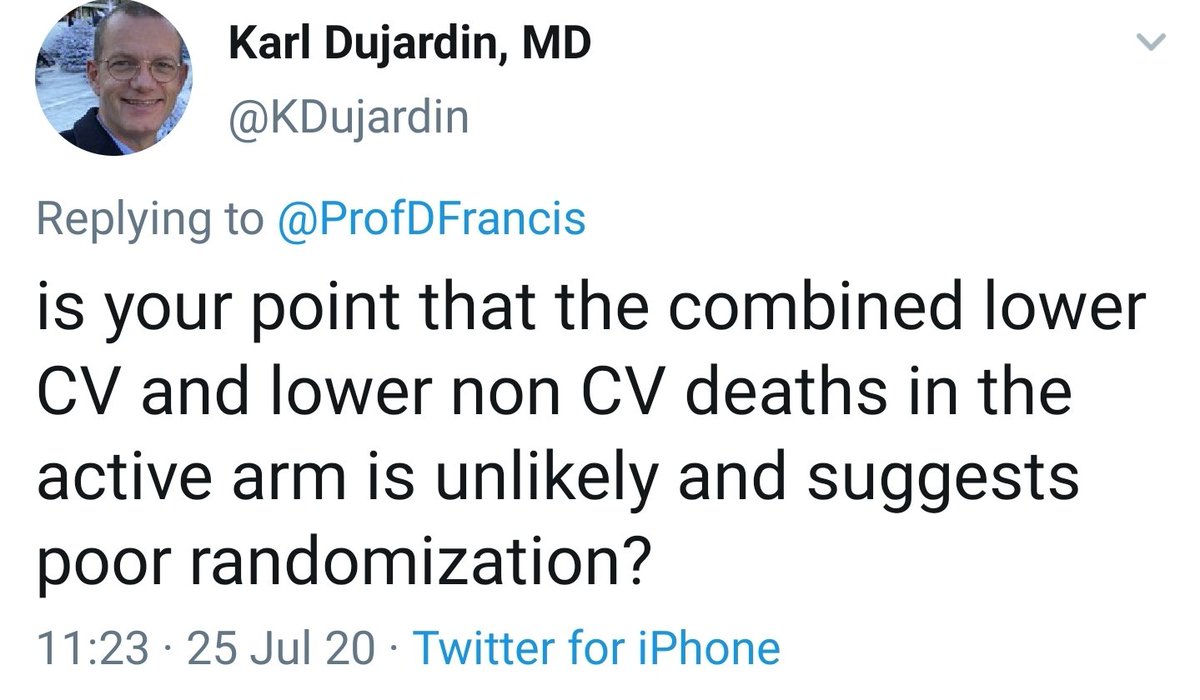
Sorry I may have got so excited that I didn't explain fully.
When you prevent CV death, you are always anxious that you don't cause non-CV death.
For example, if you give people antihypertensives, you might prevent strokes etc, but cause more hypotension and resultant falls etc.
For example, if you give people antihypertensives, you might prevent strokes etc, but cause more hypotension and resultant falls etc.
Remember the Perioperative Beta Blockade fiasco presided over by the ESC?
Initiating perioperative beta blockade DEFINITELY prevents MI, and deaths due to MI.
But it also increases other causes of death. By much more.
So total death goes up.
Initiating perioperative beta blockade DEFINITELY prevents MI, and deaths due to MI.
But it also increases other causes of death. By much more.
So total death goes up.
Moreover suppose you give ANY drug that just causes some fatal side effect outside the Cardiovascular system.
That would prevent cardiovascular death (because people who have died early because of the side effect, don't then live long enough to get their CV death)
That would prevent cardiovascular death (because people who have died early because of the side effect, don't then live long enough to get their CV death)
The way we would detect that is that non-CV deaths would go up.
That way we know we have either
(a) reclassified CV deaths as non-CV
or even
(b) caused more non-CV deaths than the CV deaths we prevent.
That way we know we have either
(a) reclassified CV deaths as non-CV
or even
(b) caused more non-CV deaths than the CV deaths we prevent.
So trials generally check that NON-CV deaths don't get increased, as that is the fear.
However, we never find that NON-CV deaths get DECREASED. That would be too amazingly good.
However, we never find that NON-CV deaths get DECREASED. That would be too amazingly good.
Any competent fraudster would make sure that the non-CV deaths are roughly unchanged, or even slightly increased, so that they could say "It saves lives, at only a small cost" and that way seem plausible.
However these guys obviously didn't check the non-CV death totals, so they didn't realise the implication of their made-up data.
What they accidentally reported was a treatment (moving one of your BP tablets to the night) that reduced NON-CV deaths by 39%!
Wow!
What do people die of, other than CV death?
Mainly cancer.
Plus a few other things.
What do people die of, other than CV death?
Mainly cancer.
Plus a few other things.
So if you really could reduce non-CV death by 39%, by just tweaking the timing of a BP tablet, you wouldn't publish it in EHJ.
You would publish it in a major *general* journal, e.g. Lancet / NEJM / JAMA
Or even the Bible.
You would publish it in a major *general* journal, e.g. Lancet / NEJM / JAMA
Or even the Bible.
It would be an unimaginably large effect for a ridiculously small intervention with no pre-existing biological basis.
They wouldn't just give old Hermida the Nobel Prize.
They wouldn't just give old Hermida the Nobel Prize.
They would fly over to his house and make him Emperor of Sweden.
They would cancel the next 10 years of Nobels, and say all those medals would all be awarded to him.
THAT is how unbelievably amazing it is.
They would cancel the next 10 years of Nobels, and say all those medals would all be awarded to him.
THAT is how unbelievably amazing it is.
And he didn't even mention it in the paper.
So he is either very modest.
Or didn't notice in his hasty fakery.
I think the latter. He is not only a fraudster, but an outstandingly incompetent one.
So he is either very modest.
Or didn't notice in his hasty fakery.
I think the latter. He is not only a fraudster, but an outstandingly incompetent one.
And if I really did know Swedish I would have realised what this article said.
Congrats to Mattias Brunström and Per Svensson on this:
Congrats to Mattias Brunström and Per Svensson on this:

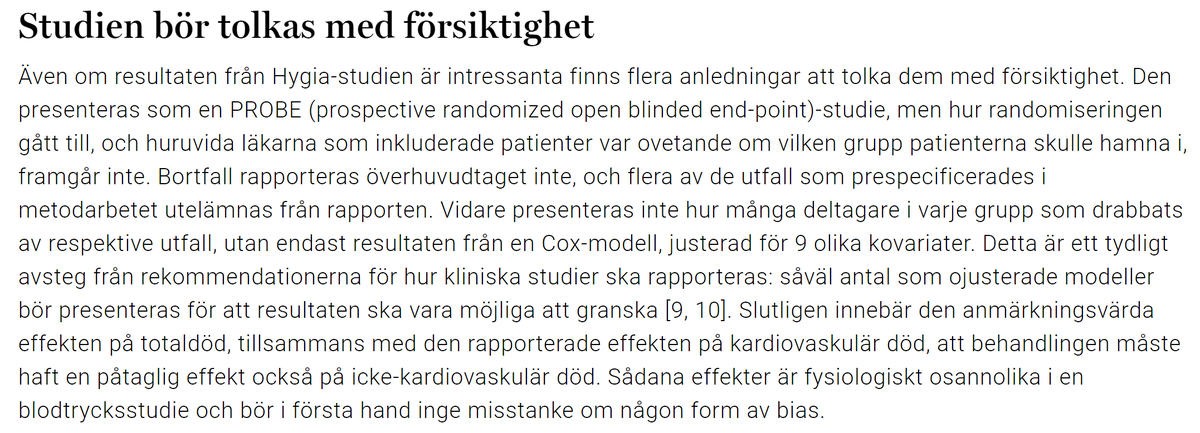
For us Brits who don't learn other languages, but instead just speak English in an increasingly loud and slow voice, this is what it means, courtesy of Google Translate:

Yup. The Swedes beat me to it.
But thankfully, due to the genius of Brexit, whereby we leave every form of civilisation behind us, and row confidently into the middle of the ocean, to slowly sink, I can proudly say,
"I am the first in my trading block (of nobody) to say this."
Thank you B Johnson and N Farage
"I am the first in my trading block (of nobody) to say this."
Thank you B Johnson and N Farage