There has been a bit of skepticism for my model's estimate that 20% of Florida (& other states) have been infected.
covid19-projections.com/us-fl
While I'm not claiming that this is necessarily true, here are some common mistakes I've seen people make when estimating true infections.
covid19-projections.com/us-fl
While I'm not claiming that this is necessarily true, here are some common mistakes I've seen people make when estimating true infections.
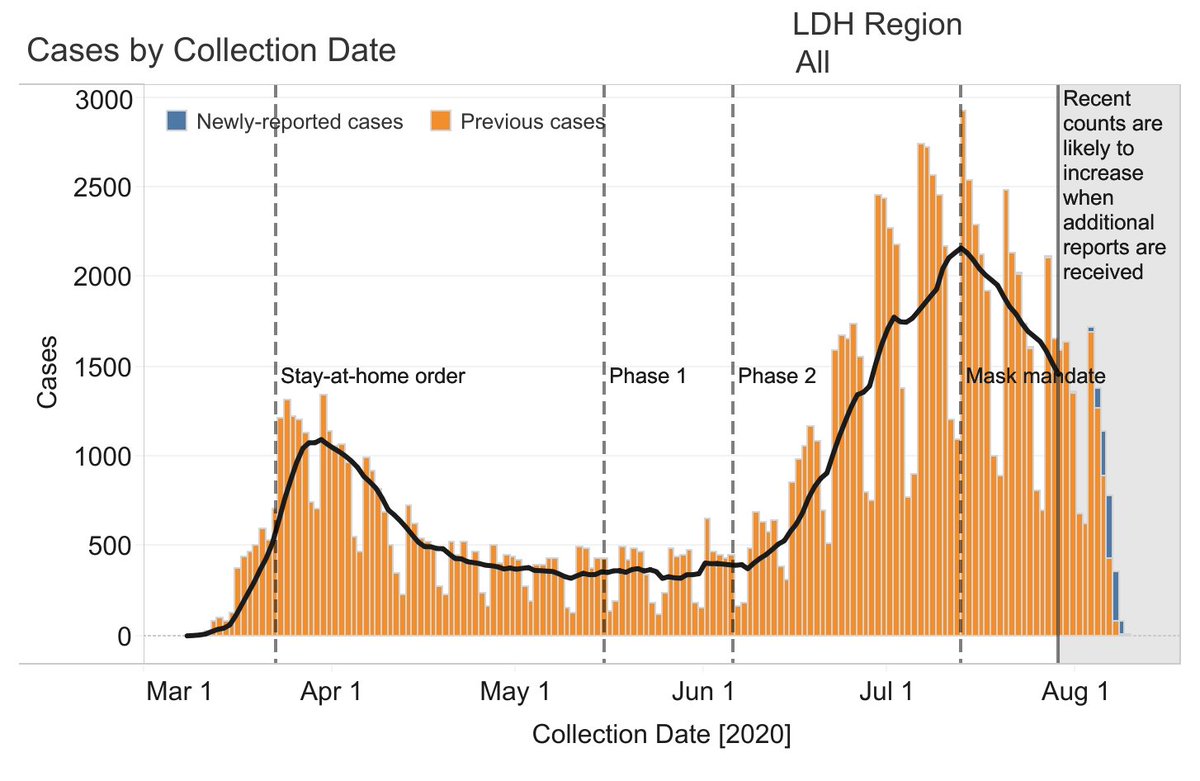
1) If we use cases and infection-to-case ratio to estimate true infections, the result we get is an estimate of the true infections from *~2 week prior*, not *right now*. This is because cases lag infections.
This matters when 1-3% of the population are being infected weekly.
This matters when 1-3% of the population are being infected weekly.
1a) Also note that the infection-to-case ratio was >10x in March/April due to lack of testing, skewing the overall ratio upwards.
Test positivity plays a role as well. At 10-20%, there is a high chance that we are missing more infections than usual.
Test positivity plays a role as well. At 10-20%, there is a high chance that we are missing more infections than usual.
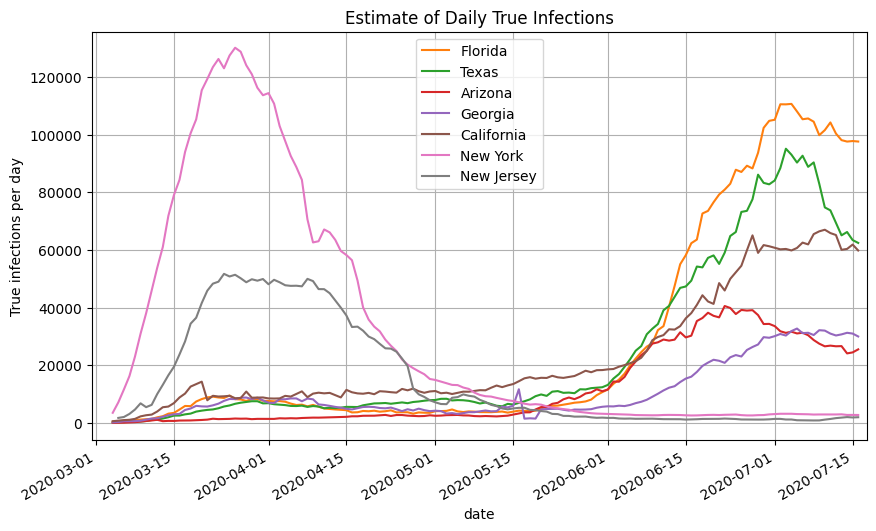
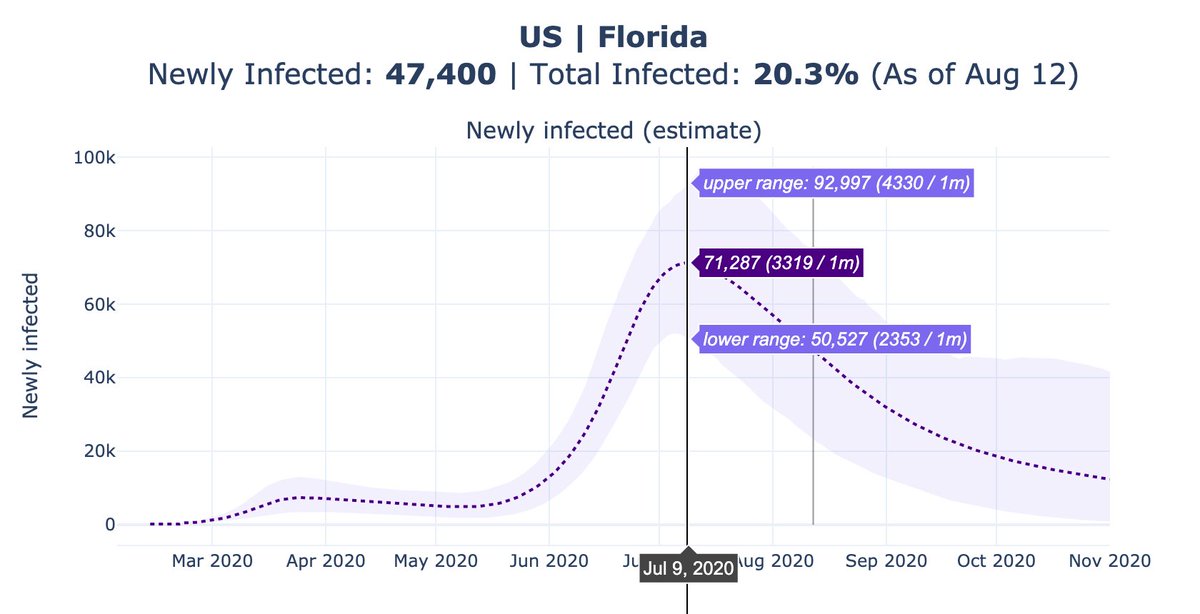
At its peak in July, Florida reported ~12,000 new cases per day. Our peak estimate for daily infections is 72,000 new infections.
The implied infection-to-case ratio is 6x. The lower bound is 4x and the upper bound is 8x.
That is largely consistent with recent findings.
The implied infection-to-case ratio is 6x. The lower bound is 4x and the upper bound is 8x.
That is largely consistent with recent findings.
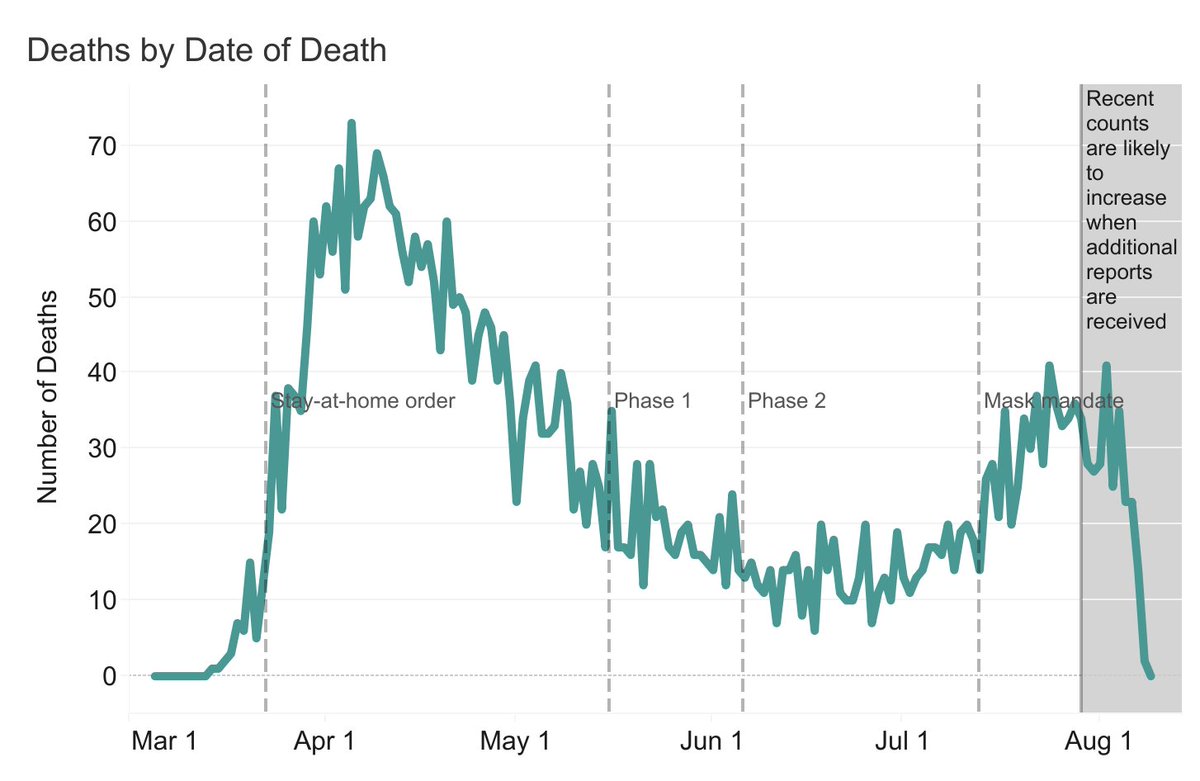
2) If we use deaths and IFR to estimate true infections, the result we get is an estimate of true infections from *~4 weeks prior*, not *right now*. This is because reported deaths lag infections.
This matters when 1-3% of the population are being infected weekly.
This matters when 1-3% of the population are being infected weekly.
2a) If we use deaths and age-adjusted IFR to estimate true infections, it's also important to account for excess deaths and the lower median age of infections.
This matters when many states are undercounting deaths and when young adults have a significantly lower fatality rate.
This matters when many states are undercounting deaths and when young adults have a significantly lower fatality rate.
A common mistake is to take 8,750 reported deaths in FL & divide by 0.5% IFR to get 1.75M, or 8% infected.
But that's how many people were infected *4 weeks ago*, under the assumptions that a) there's zero undercounting & b) age distribution of infections matches the population.
But that's how many people were infected *4 weeks ago*, under the assumptions that a) there's zero undercounting & b) age distribution of infections matches the population.
3) If we use serology studies to estimate true infections, keep in mind that a) it may take weeks to develop antibodies, b) not everyone develops detectable amount of antibodies c) sensitivity of tests vary, & d) antibodies levels may decline over time.
3a) If we use deaths and serology results from New York to benchmark infections in other states, keep in mind that the IFR for New York in March/April is 2-4x higher than the currently accepted IFR.
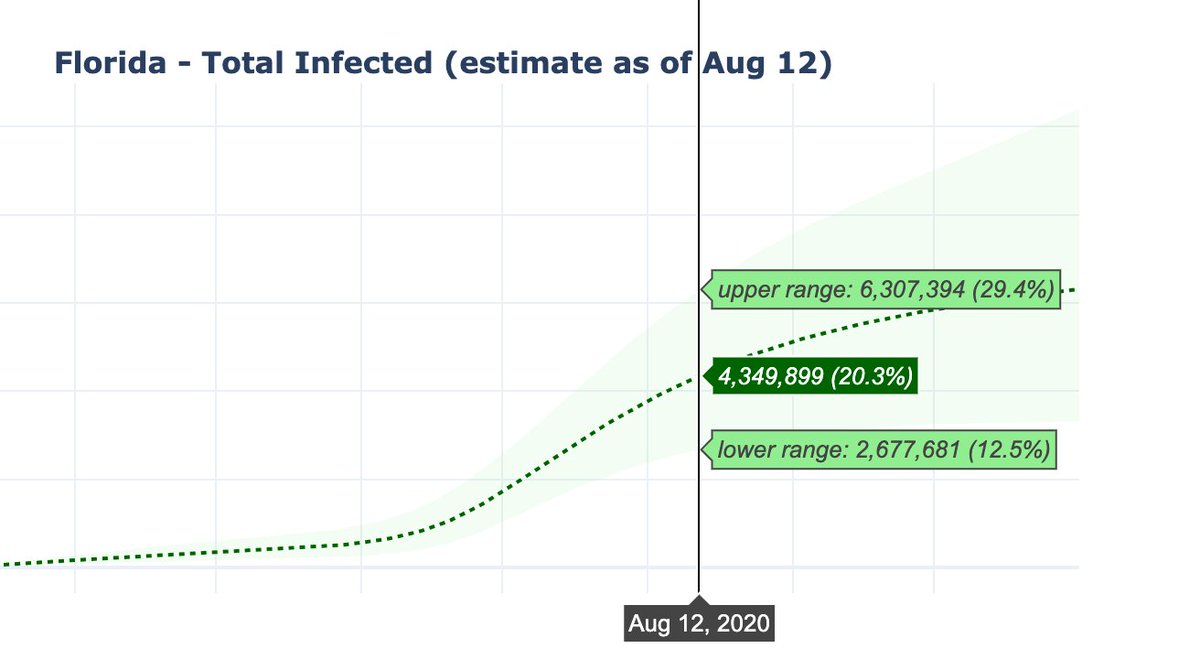
Once we factor in all of the considerations above, we find that an estimate of 12-30% infected for Florida with a mean of 20% is not unreasonable.
Could it still be too high? Sure, but the data thus far has yet to suggest otherwise. This could change as we find out more.
Could it still be too high? Sure, but the data thus far has yet to suggest otherwise. This could change as we find out more.
To conclude, there are a lot of nuances in estimating true infections in a region that can lead to a misinterpretation of the results. It's important that we take into account the inherent lag in the data.
Hopefully, this thread helps clarify these intricacies a bit better.
Hopefully, this thread helps clarify these intricacies a bit better.