
1/15: #MedTwitter: You are admitting a 50-year-old man with a hx GI bleed for a PE. You start a heparin drip. What do you titrate the drip to?
2/15: At my institution, heparin anti-Xa levels (HAL) are recommended, but we routinely draw both aPTT and HAL. I’ve always wondered WHY?
There’s also the page: “The aPTT is supra-therapeutic but the HAL is therapeutic, which should we use?”
Let’s de-mystify this!
There’s also the page: “The aPTT is supra-therapeutic but the HAL is therapeutic, which should we use?”
Let’s de-mystify this!
3/15: First, let’s understand unfractionated heparin (UFH).
UFH is a negatively charged, heterogenous mix of oligosaccharides. Heparin MUST bind antithrombin (AT) to have an anticoagulant effect. AT then inhibits Xa, thrombin (II), and other proteases.
pubmed.ncbi.nlm.nih.gov/27384570/
UFH is a negatively charged, heterogenous mix of oligosaccharides. Heparin MUST bind antithrombin (AT) to have an anticoagulant effect. AT then inhibits Xa, thrombin (II), and other proteases.
pubmed.ncbi.nlm.nih.gov/27384570/

4/15: Heparin frequently uncouples from AT & also binds to other plasma proteins. Only a third of the administered UFH is the minimum length needed to bind AT and inhibit thrombin. All this leads to variable anticoagulation response and the need for therapeutic monitoring.
5/15: What is the aPTT? PTT measures intrinsic & common clotting pathways integrity. For citrated plasma to clot in vitro, it needs a reagent of: phospholipid + an activator (speeds up clot time), the “a” in 𝗮PTT. After incubation, calcium is added and the clot time is measured.
6/15: There’s immense heterogeneity in reagents, centrifuge speed, incubation time, and clot detection techniques. Ergo, the aPTT is not a standardized assay and the “therapeutic range” can vary between laboratories.
7/15 Also, aPTT is affected by acute phase reactants, factor deficiencies, liver disease, which can lead to over/under coagulation during titration.
8/15 All this⬆️has led to some hospitals to use anti-Xa levels instead. My hospital calls this a “HAL”: it is essentially an anti-Xa level using a heparin-specific reagent.
How is HAL obtained?
How is HAL obtained?
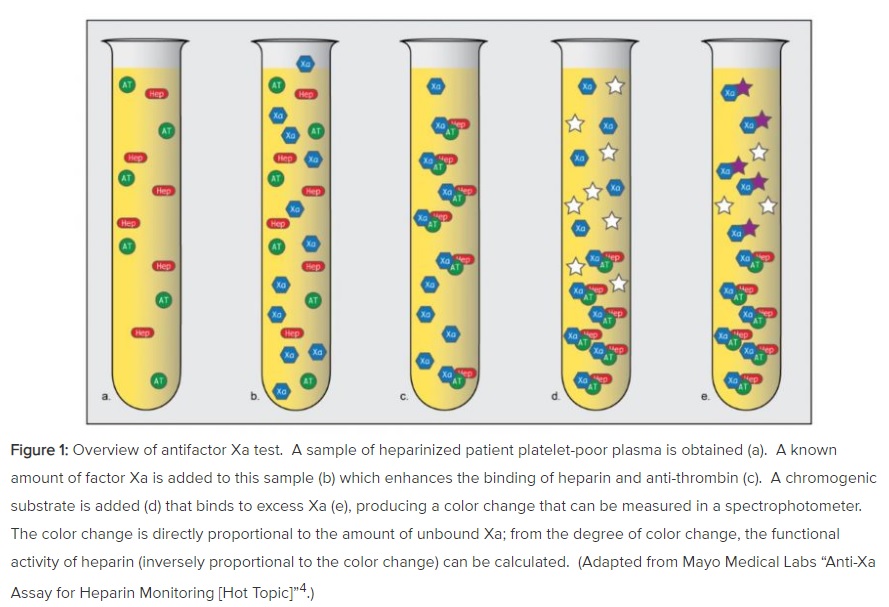
9/15: A known amount of Xa is added to your patient’s heparinzed plasma. Remember: heparin binds AT. This complex inhibits the Xa you just added. The degree of inhibition is the heparin activity level. This value is obtained via a chromogenic assay:
tinyurl.com/yyrwbhk4
tinyurl.com/yyrwbhk4
10/15 So, The HAL is a measure of heparin activity 𝗮𝗴𝗮𝗶𝗻𝘀𝘁 𝗳𝗮𝗰𝘁𝗼𝗿 𝗫𝗮 𝗼𝗻𝗹𝘆 and NOT of your overall hemostasis, unlike aPTT.
11/15 HAL is less affected by biologic factors and technique. When compared to aPTT, titration to HAL leads to quicker time to therapeutic range, fewer rate adjustments, less heparin exposure and is cost-neutral. This had led to many hospitals favoring HAL > aPTT.
12/15: What do you do when the aPTT and HAL are DISCORDANT? Price et. al found that aPTT and HAL agreed only 40% of the time in hospitalized patients on UFH!
pubmed.ncbi.nlm.nih.gov/23386070
pubmed.ncbi.nlm.nih.gov/23386070
13/15: They also looked at a group of patients who had 2 consecutive measurements of disproportionately high aPTT to HAL while receiving UFH: this group had much higher rates of 21-day major-bleeding.
What is the verdict? Which is better?
What is the verdict? Which is better?
14/15: It depends:
1. When aPTT and HAL are concordant, go w/ HAL: fewer adjustments & quicker time to therapeutic range.
2. When aPTT is discordantly high vs. HAL, your pt may be at higher risk for major bleed. Work to reduce bleeding risk (titrate to aPTT or lower HAL).
1. When aPTT and HAL are concordant, go w/ HAL: fewer adjustments & quicker time to therapeutic range.
2. When aPTT is discordantly high vs. HAL, your pt may be at higher risk for major bleed. Work to reduce bleeding risk (titrate to aPTT or lower HAL).
15/15: Takeaways:
1. aPTT provides a better global assessment of hemostasis but is finicky.
2. aPTT and HAL are frequently discordant in the hospitalized patient.
3. If aPTT is discordantly ⬆️ vs. HAL, pts are at higher risk for bleeding. Consider using aPTT or a lower HAL.
1. aPTT provides a better global assessment of hemostasis but is finicky.
2. aPTT and HAL are frequently discordant in the hospitalized patient.
3. If aPTT is discordantly ⬆️ vs. HAL, pts are at higher risk for bleeding. Consider using aPTT or a lower HAL.

