1/ Allyship & Upstanding = Inclusion 2.0
Last week you learned how to create a safe and welcoming learning environment.
Today we make sure that is true for every identity that someone brings to our team.
Last week you learned how to create a safe and welcoming learning environment.
Today we make sure that is true for every identity that someone brings to our team.
2.1/ These terms may be new to some of you. So what am I talking about?
⭐️ Allyship = the practice of emphasizing social justice, inclusion, and human rights by members of an ingroup, to advance the interests of an oppressed or marginalized outgroup.
⭐️ Allyship = the practice of emphasizing social justice, inclusion, and human rights by members of an ingroup, to advance the interests of an oppressed or marginalized outgroup.
2.2/
⭐️ Upstanding = speaking up when being a bystander (one who is present, but not taking part in a situation or event).
⭐️ Upstanding = speaking up when being a bystander (one who is present, but not taking part in a situation or event).
3/ Another way to distinguish these ideas is:
✅ Allyship is the attitude we need to assume when leading a team (but preferably, this is an “all-day-everyday” thing).
✅ Upstanding is the action we must do when anyone on our team experiences a microaggression.
✅ Allyship is the attitude we need to assume when leading a team (but preferably, this is an “all-day-everyday” thing).
✅ Upstanding is the action we must do when anyone on our team experiences a microaggression.
4/ Let’s be clear what a microaggression is. See the photo for the definition per an expert on microaggressions.
📝: It is an imperfect term. Some think it is too harsh. Others feel it is a diminution of traumatic experiences.
📝: It is an imperfect term. Some think it is too harsh. Others feel it is a diminution of traumatic experiences.

5/ Are microaggressions part of clinical medicine?
Uh…YEAH!
👀 this paper that is 🔥 & hot off the presses in @AcadMedJournal from: @jbullockruns & @karenhauer4
TL;DR. Stereotype Threat (a result of microaggressions) is common & interferes with learning. Allyship could help!
Uh…YEAH!
👀 this paper that is 🔥 & hot off the presses in @AcadMedJournal from: @jbullockruns & @karenhauer4
TL;DR. Stereotype Threat (a result of microaggressions) is common & interferes with learning. Allyship could help!
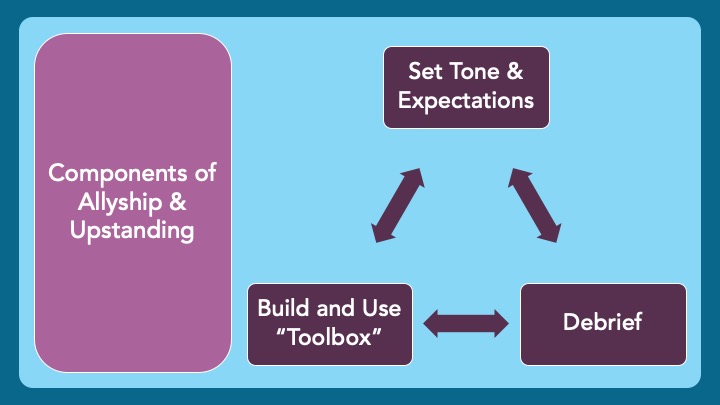
6/ So, let’s get practical. There are three parts to allyship and upstanding (H/T @WheelerMed & @DrCalvinChou):
1⃣ Set the Tone & Expectations (allyship)
2⃣ Use your “toolbox” (upstanding)
3⃣ Debrief (allyship)
Let's dive into each of these key pieces.
1⃣ Set the Tone & Expectations (allyship)
2⃣ Use your “toolbox” (upstanding)
3⃣ Debrief (allyship)
Let's dive into each of these key pieces.
7/ Caveat: I identify as a white, cis-gender, heterosexual male physician.
The Venn Diagram of my identities & the groups that hold power in medicine is a ⭕️.
For me, and people like me, being all about allyship and upstanding needs to be of paramount importance.
The Venn Diagram of my identities & the groups that hold power in medicine is a ⭕️.
For me, and people like me, being all about allyship and upstanding needs to be of paramount importance.
8/ Those who identify as underrepresented in medicine (UIM) can also be allies and upstand
Medical training & the roles you accumulate (resident, fellow, attending, etc.) confer power
Power is a responsibility to create psychological safety for trainees. Anyone can be an ally!
Medical training & the roles you accumulate (resident, fellow, attending, etc.) confer power
Power is a responsibility to create psychological safety for trainees. Anyone can be an ally!
9/ Step 1: Setting the Tone and Expectations.
4 things to do here:
1⃣ Let it be known that microaggressions happen
2⃣ Pledge to be an ally to trainees in addressing microaggressions
3⃣ Discuss how your trainees want you to upstand
4⃣ Discuss lenses and your fallibility
4 things to do here:
1⃣ Let it be known that microaggressions happen
2⃣ Pledge to be an ally to trainees in addressing microaggressions
3⃣ Discuss how your trainees want you to upstand
4⃣ Discuss lenses and your fallibility

10.1/ Step 1.3 - Upstanding can be done in many ways, but it is key to ask learners what they want from you as a supervisor.
Do THEY want to upstand for themselves? Do they want YOU to take charge? Do they want things addressed directly? Or something more subtle?
Do THEY want to upstand for themselves? Do they want YOU to take charge? Do they want things addressed directly? Or something more subtle?
10.2/ Allyship and upstanding is about feeling safe. How that is best accomplished is unique to each person.
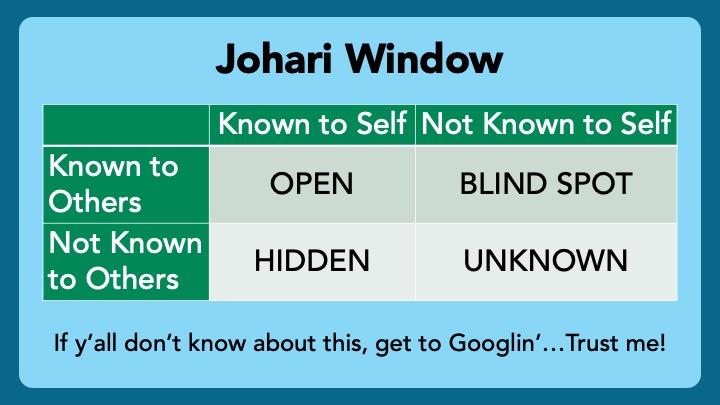
11/ Step 1.4 - We each see the world through our unique lenses. You will not see all microaggressions. You can’t.
You CAN be explicit and acknowledge that you will miss some things, but you want to be notified when this happens.
Ask for all the feedback you can get!
You CAN be explicit and acknowledge that you will miss some things, but you want to be notified when this happens.
Ask for all the feedback you can get!
12/ OK. Groundwork laid. Team is cruising along. Microaggression occurs. What now?
Step 2: You need a “toolbox” of ways to intervene. There are plenty of resources out there to build your toolbox.
Here are a few articles to get you started. Links in the following tweet.
Step 2: You need a “toolbox” of ways to intervene. There are plenty of resources out there to build your toolbox.
Here are a few articles to get you started. Links in the following tweet.

12.1/ Links to Toolbox articles…
@WheelerMed et al. in @MedTeachJournal: pubmed.ncbi.nlm.nih.gov/30277121/
@MadelineBTorres et al. in @JAMASurgery: pubmed.ncbi.nlm.nih.gov/31290954/
Paul-Emile et al. in @NEJM: pubmed.ncbi.nlm.nih.gov/26933847/
@WheelerMed et al. in @MedTeachJournal: pubmed.ncbi.nlm.nih.gov/30277121/
@MadelineBTorres et al. in @JAMASurgery: pubmed.ncbi.nlm.nih.gov/31290954/
Paul-Emile et al. in @NEJM: pubmed.ncbi.nlm.nih.gov/26933847/
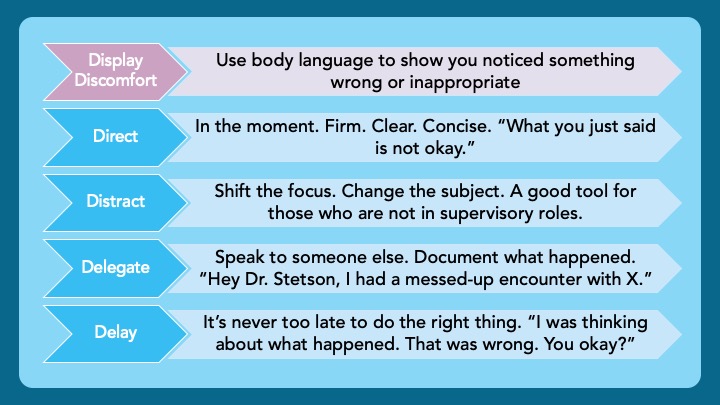
14/ A simple and memorable toolbox comes courtesy of @gradydoctor. Behold, the ”5 Ds"
Discuss these options with your team. This way, they can choose tools for themselves, and the ones they hope you can employ.
Link to Dr. Manning's Grand Rounds:
Discuss these options with your team. This way, they can choose tools for themselves, and the ones they hope you can employ.
Link to Dr. Manning's Grand Rounds:
15/ Step 3: DEBRIEF
Arguably, this is the most important part.
Regardless of how well you performed in the moment, always take the time to reflect.
“That was really uncomfortable for me. I know I didn’t handle it perfectly. How are you all feeling?”
Arguably, this is the most important part.
Regardless of how well you performed in the moment, always take the time to reflect.
“That was really uncomfortable for me. I know I didn’t handle it perfectly. How are you all feeling?”
16/ This is also a great time to display a Growth Mindset and get feedback from the group about how you can be a better upstander for the next time.
”I am not sure I handled that in the best way. What do you all think I could have done better in that situation?”
”I am not sure I handled that in the best way. What do you all think I could have done better in that situation?”
17/ Summary Slide! Three steps to Allyship and Upstanding:
1⃣ Set the Tone & Expectations (allyship)
2⃣ Use your “toolbox” (upstanding) - "5 Ds"
3⃣ DEBRIEF (allyship)
Thanks for engaging in this important topic. Please, let us know your thoughts by commenting on this thread.
1⃣ Set the Tone & Expectations (allyship)
2⃣ Use your “toolbox” (upstanding) - "5 Ds"
3⃣ DEBRIEF (allyship)
Thanks for engaging in this important topic. Please, let us know your thoughts by commenting on this thread.

18/ Join us next week as @JenniferSpicer4 helps us negotiate the “work vs. learning” paradigm and think about the best ways to make ourselves available to our learners.
All our threads are available @MedEdTwagTeam. Give us a follow and check out the previous Tweetorials.
All our threads are available @MedEdTwagTeam. Give us a follow and check out the previous Tweetorials.
• • •
Missing some Tweet in this thread? You can try to
force a refresh