
I am quarantined in London, so #Tweetorial time💂♂️⏰
Should we treat subclinical hypothyroidism during pregnancy?
A tweetorial on physiology, overdiagnosis, risk stratification and treatment harms.
Do you treat subclinical hypothyroidism during pregnancy?❌✅
Should we treat subclinical hypothyroidism during pregnancy?
A tweetorial on physiology, overdiagnosis, risk stratification and treatment harms.
Do you treat subclinical hypothyroidism during pregnancy?❌✅
Subclinical hypothyroidism [⬆️TSH, ↔️FT4] occurs in ~3.5% of pregnancies.
- Short differential (fig)
- No/Mild symptomatology overlaps with pregnancy, doesn't distinguish
- Consistent associations of modestly increased risk of miscarriage, preterm birth and low birth weight.
- Short differential (fig)
- No/Mild symptomatology overlaps with pregnancy, doesn't distinguish
- Consistent associations of modestly increased risk of miscarriage, preterm birth and low birth weight.

First, how to get the diagnosis right?
- Use of the correct reference range is pivotal (grey area of figure).
So, do not use 2.5/3.0 mU/L cut-offs
Note: Any TSH above 10 mU/L = overt hypothyroidism (or lab artefact)
liebertpub.com/doi/full/10.10…
- Use of the correct reference range is pivotal (grey area of figure).
So, do not use 2.5/3.0 mU/L cut-offs
Note: Any TSH above 10 mU/L = overt hypothyroidism (or lab artefact)
liebertpub.com/doi/full/10.10…

Incorrect reference range ➡️ overdiagnosis of approximately 1 in every 9 patients (fig)
Overdiagnosis ➡️ overtreatment ➡️ increased risk of harm
Note: plenty of data on BMI/ethnicity ref ranges, but no evidence this is clinically meaningful
liebertpub.com/doi/abs/10.108…
Overdiagnosis ➡️ overtreatment ➡️ increased risk of harm
Note: plenty of data on BMI/ethnicity ref ranges, but no evidence this is clinically meaningful
liebertpub.com/doi/abs/10.108…

However, you need FT4 for your diagnosis as well..
Large inter assay differences in FT4 do not allow guidelines to provide any fixed FT4 limits
Best option = adopt a ref range from literature
Why not use the total T4 instead?
Large inter assay differences in FT4 do not allow guidelines to provide any fixed FT4 limits
Best option = adopt a ref range from literature
Why not use the total T4 instead?
Bad idea:
- >99% = bound
Thus: biologically unavailable & reflection of TBG/estrogen
- Literature on ref ranges very poor (very poor data for 150% of non-pregnancy ref range)
- Poor reflection of HPT axis (fig)
- No associations with adverse outcomes
pubmed.ncbi.nlm.nih.gov/27187054/
- >99% = bound
Thus: biologically unavailable & reflection of TBG/estrogen
- Literature on ref ranges very poor (very poor data for 150% of non-pregnancy ref range)
- Poor reflection of HPT axis (fig)
- No associations with adverse outcomes
pubmed.ncbi.nlm.nih.gov/27187054/

Back to subhypo, why care?
Because it is opposite of normal physiology (fig):
hCG➡️TSH receptor stimulation➡️FT4⬆️& TSH⬇️
Also, hCG➡️pituitary TSH receptor stimulation➡️ultrashort feedback loop➡️TSH suppression
AKA the Brokken-Wiersinga-Prummel Loop pubmed.ncbi.nlm.nih.gov/15588378/
Because it is opposite of normal physiology (fig):
hCG➡️TSH receptor stimulation➡️FT4⬆️& TSH⬇️
Also, hCG➡️pituitary TSH receptor stimulation➡️ultrashort feedback loop➡️TSH suppression
AKA the Brokken-Wiersinga-Prummel Loop pubmed.ncbi.nlm.nih.gov/15588378/

Women with gestational subclinical hypothyroidism exhibit a decreased thyroid functional capacity.
Upper: no association of hCG with subhypo
Lower: no FT4 increase with higher hCG in subhypo
Upper: no association of hCG with subhypo
Lower: no FT4 increase with higher hCG in subhypo

Why?
- Thyroid autoimmunity: 1/3 of women with subhypo are TPOAb positive ➡️ impaired thyroidal response to hCG (upper fig)
Yet, also TPOAb neg subhypo no association with hCG (lower left). Other subhypo risk factors (upper right) or other causes may play a role.
- Thyroid autoimmunity: 1/3 of women with subhypo are TPOAb positive ➡️ impaired thyroidal response to hCG (upper fig)
Yet, also TPOAb neg subhypo no association with hCG (lower left). Other subhypo risk factors (upper right) or other causes may play a role.

So, to treat or not to treat?
Risk stratification is key!
Below: overview of ATA guidelines (green = no treatment, red = treatment).
We’ll get to gray zone..
liebertpub.com/doi/full/10.10…
Risk stratification is key!
Below: overview of ATA guidelines (green = no treatment, red = treatment).
We’ll get to gray zone..
liebertpub.com/doi/full/10.10…

Risk stratification using TPOAb status is based on abnormal physiology (above) + small RCT (to follow)
Also on observational studies that show: high TSH + TPOAb positivity = high-risk group (examples below).
Also on observational studies that show: high TSH + TPOAb positivity = high-risk group (examples below).

How about RCTs of levothyroxine treatment?
1 positive, showing lower risk preterm birth (below)
Note: study started with old ref ranges, LT4 benefit for TSH >4 is another argument for use of current ref ranges
pubmed.ncbi.nlm.nih.gov/27879326/
pubmed.ncbi.nlm.nih.gov/29126290/
1 positive, showing lower risk preterm birth (below)
Note: study started with old ref ranges, LT4 benefit for TSH >4 is another argument for use of current ref ranges
pubmed.ncbi.nlm.nih.gov/27879326/
pubmed.ncbi.nlm.nih.gov/29126290/

Other RCTs did not risk stratification:
- 1 (over)treated (150ug/day), start week 13
- 1 treated with 75ug/day, start week 18
Based on RCTs:
- Still unsure if treatment is beneficial
- If you treat: start early, don’t overtreat
nejm.org/doi/full/10.10…
nejm.org/doi/full/10.10…
- 1 (over)treated (150ug/day), start week 13
- 1 treated with 75ug/day, start week 18
Based on RCTs:
- Still unsure if treatment is beneficial
- If you treat: start early, don’t overtreat
nejm.org/doi/full/10.10…
nejm.org/doi/full/10.10…
How about that grey zone?
Guidelines: consider treatment, individualize
Think about:
- Abnormal physiology: subhypo despite high hCG (twin, 8-11 wks)
- High TSH
- High-normal TPOAb titer (academic.oup.com/jcem/article/1…)
- High pretest probability of subhypo related adverse outcomes
Guidelines: consider treatment, individualize
Think about:
- Abnormal physiology: subhypo despite high hCG (twin, 8-11 wks)
- High TSH
- High-normal TPOAb titer (academic.oup.com/jcem/article/1…)
- High pretest probability of subhypo related adverse outcomes

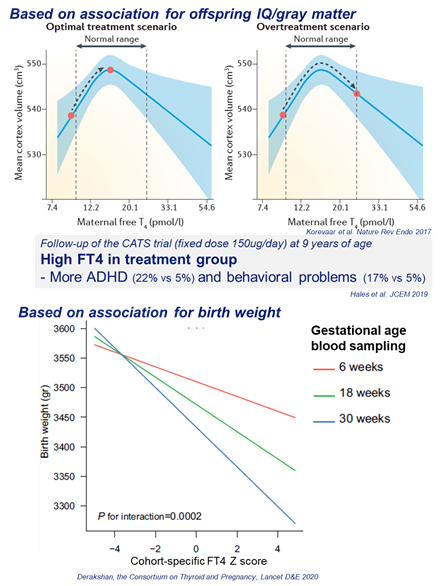
If you decide to treat:
Beware of overtreatment!
High FT4 associated with lower birth weight, child IQ and cerebral gray mass (fig).
For example start with 50ug daily and titrate after 2-4 weeks
Beware of overtreatment!
High FT4 associated with lower birth weight, child IQ and cerebral gray mass (fig).
For example start with 50ug daily and titrate after 2-4 weeks
Subclinical hypothyroidism during pregnancy:
* Reflects an abnormal physiology
* Use correct reference ranges to diagnose
* Risk stratify: TPOAbs, gestational age etc.
* If you treat ➡️ Don’t overtreat
* Reflects an abnormal physiology
* Use correct reference ranges to diagnose
* Risk stratify: TPOAbs, gestational age etc.
* If you treat ➡️ Don’t overtreat
I hope this was useful!
For other very good tweetorials, follow those who inspired me
@tony_breu
@CPSolvers
@ebtapper
@ash_bo21
@AvrahamCooperMD
@MiddeldorpS
@Leo_ReapDO
#thyroidchat
More time to spare?
A hyperthyroidism tweetorial:
For other very good tweetorials, follow those who inspired me
@tony_breu
@CPSolvers
@ebtapper
@ash_bo21
@AvrahamCooperMD
@MiddeldorpS
@Leo_ReapDO
#thyroidchat
More time to spare?
A hyperthyroidism tweetorial:
Typo! The second outcome is preterm birth, not miscarriage.



