1/
55M prev healthy developed gait instability and tremor about 2 months ago. He later starting dropping items due to jerking movements and had word-finding difficulties. Family brought him in due to falls and worsening mood changes.
EEG with periodic sharp wave complexes
MRI 👇
55M prev healthy developed gait instability and tremor about 2 months ago. He later starting dropping items due to jerking movements and had word-finding difficulties. Family brought him in due to falls and worsening mood changes.
EEG with periodic sharp wave complexes
MRI 👇

2/
An LP is done ➡️ Which of these studies will be most helpful for diagnosis?
#IDTwitter #MedTwitter #IDMedEd @ID_fellows
An LP is done ➡️ Which of these studies will be most helpful for diagnosis?
#IDTwitter #MedTwitter #IDMedEd @ID_fellows
3/
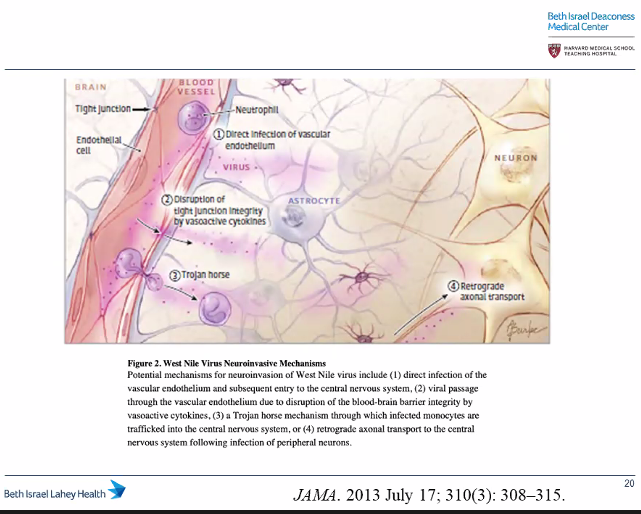
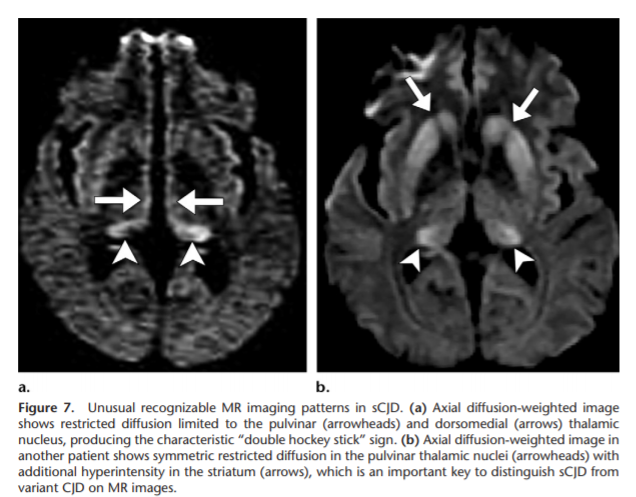
Ultimate dx was Creutzfeldt-Jakob disease!
Can see "pulvinar" (posterior thalami) or "double hockey stick" (dorsomedial thalami) signs on T2-wt'd, FLAIR, diffusion-wt'd MRI
Image ref + comprehensive review of imaging with CJD: pubs.rsna.org/doi/10.1148/rg…
Ultimate dx was Creutzfeldt-Jakob disease!
Can see "pulvinar" (posterior thalami) or "double hockey stick" (dorsomedial thalami) signs on T2-wt'd, FLAIR, diffusion-wt'd MRI
Image ref + comprehensive review of imaging with CJD: pubs.rsna.org/doi/10.1148/rg…
4/
Thanks @vdbPolly for tackling CJD in case conf this wk!
⭐️Prion infection aka Transmissable spongiform encephalopathies⭐️
▪️Neurodegen dz w/long incubation period➡️rapid progression once sxx appear
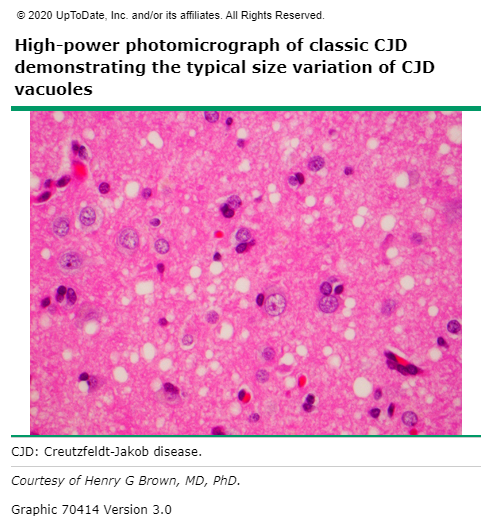
▪️Neuropathologic triad: spongioform change, neuron loss w/o inflam, gliosis
Thanks @vdbPolly for tackling CJD in case conf this wk!
⭐️Prion infection aka Transmissable spongiform encephalopathies⭐️
▪️Neurodegen dz w/long incubation period➡️rapid progression once sxx appear
▪️Neuropathologic triad: spongioform change, neuron loss w/o inflam, gliosis
5/
🔸3 categories 👇
🟩Sporadic Creutzfeldt Jakob disease (sCJD) most well-known, >90% of sporadic prion dz
◾️1 case / 1 mill pop
◾️Exact pathogenesis unknown
◾️Mean age onset ~62, range 45-75
◾️70% die in under 6 months
🟩Variant CJD
◾️Mean age ~25
🟩Iatrogenic CJD
◾️More later
🔸3 categories 👇
🟩Sporadic Creutzfeldt Jakob disease (sCJD) most well-known, >90% of sporadic prion dz
◾️1 case / 1 mill pop
◾️Exact pathogenesis unknown
◾️Mean age onset ~62, range 45-75
◾️70% die in under 6 months
🟩Variant CJD
◾️Mean age ~25
🟩Iatrogenic CJD
◾️More later

6/
Clinical:
🔹Neuropsych sxs
🔹Myoclonus, esp provoked by startle
🔹Cerebellar manifestations
🔹Corticospinal tract involvement
🔹Extrapyramidal signs
Common = rapid neuropsych decline, death w/i 1 yr
Atypical = CN abnormalities, peripheral NS involvement
Clinical:
🔹Neuropsych sxs
🔹Myoclonus, esp provoked by startle
🔹Cerebellar manifestations
🔹Corticospinal tract involvement
🔹Extrapyramidal signs
Common = rapid neuropsych decline, death w/i 1 yr
Atypical = CN abnormalities, peripheral NS involvement

7/
Evaluation:
🔸MRI discussed previously
🔸EEG: periodic sharp wave complexes
🔸Neuropath = gold standard
🔸CSF protein markers:
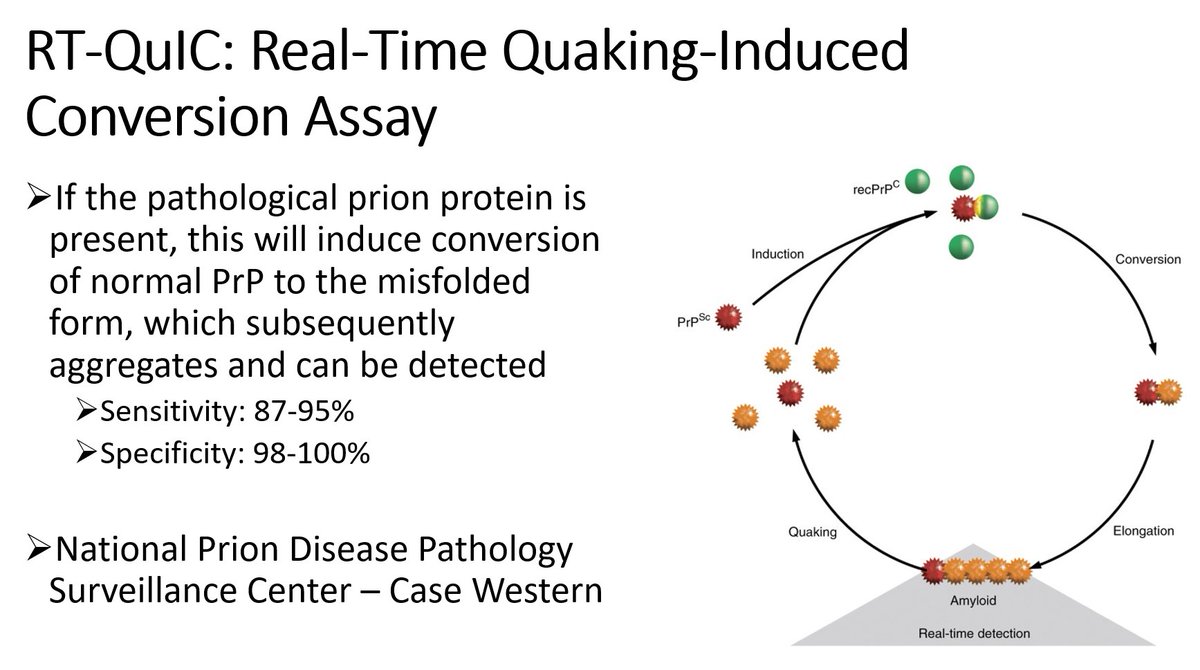
▪️RT-QuIC *most sensitive/specific*
▪️14-3-3 protein
▪️Tau protein
Evaluation:
🔸MRI discussed previously
🔸EEG: periodic sharp wave complexes
🔸Neuropath = gold standard
🔸CSF protein markers:
▪️RT-QuIC *most sensitive/specific*
▪️14-3-3 protein
▪️Tau protein
8/
@vdbPolly gave a quick review of RT-QuIC assay = real-time quaking induced conversion
pubmed.ncbi.nlm.nih.gov/22926858/
@vdbPolly gave a quick review of RT-QuIC assay = real-time quaking induced conversion
pubmed.ncbi.nlm.nih.gov/22926858/
9/
Prognosis/Tx/Prevention:
🔸Supportive/sx
🔸Palliative care as invariably fatal
🔶Iatrogenic transmission of CJD has been reported; linked to HGH, dura mater, corneal grafts, nsgy equipment
🔸No evidence of 🧍➡️🧍: ok for standard precautions for pt
Prognosis/Tx/Prevention:
🔸Supportive/sx
🔸Palliative care as invariably fatal
🔶Iatrogenic transmission of CJD has been reported; linked to HGH, dura mater, corneal grafts, nsgy equipment
🔸No evidence of 🧍➡️🧍: ok for standard precautions for pt
10/
🔸Effective decontamination paramount to ⬇️surg transmission CJD
🔸Destroy heat-resistant surg instruments in contact with high infectivity tissue (brain, spinal cord, cranial nerves, eyes)
🔸More on infection control measures➡️
who.int/csr/resources/…
cdc.gov/prions/cjd/inf…
🔸Effective decontamination paramount to ⬇️surg transmission CJD
🔸Destroy heat-resistant surg instruments in contact with high infectivity tissue (brain, spinal cord, cranial nerves, eyes)
🔸More on infection control measures➡️
who.int/csr/resources/…
cdc.gov/prions/cjd/inf…
11/
Thanks to our guest from BIDMC Neurology Dr. Greenstein! Her key take home pearls for recognizing CJD as ID doc:
1⃣⭐️timeline! Pts go downhill fast
2⃣Myoclonus (antigravity, rapid jerking mvts)
3⃣CJD=predominantly parenchymal dz, which is why CN neuropathy is atypical
Thanks to our guest from BIDMC Neurology Dr. Greenstein! Her key take home pearls for recognizing CJD as ID doc:
1⃣⭐️timeline! Pts go downhill fast
2⃣Myoclonus (antigravity, rapid jerking mvts)
3⃣CJD=predominantly parenchymal dz, which is why CN neuropathy is atypical