
1/ Reports that Trump received #dexamethasone— a steroid that should only be used on patients who require oxygen or are critically ill with #covid19. This was proven to reduce mortality in the RECOVERY trial published in @NEJM earlier this year.
nejm.org/doi/full/10.10…
nejm.org/doi/full/10.10…
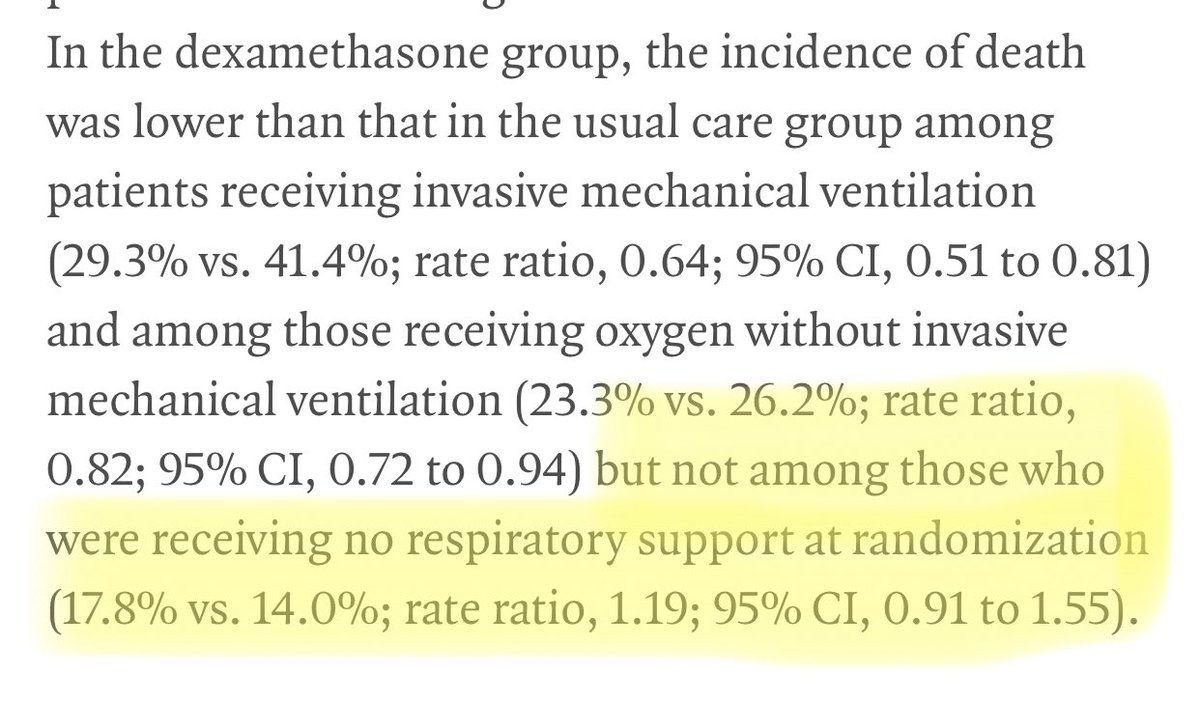
2/ But, they found no mortality benefit in patients that were not on supplemental oxygen or ventilators.
In fact, those patients actually had a slightly higher mortality rate, although not statistically significant.
In fact, those patients actually had a slightly higher mortality rate, although not statistically significant.
3/ The basic premise is that once you are sick enough, your immune response is what needs to be tempered/ what may end up killing you rather than the virus itself. So steroids can help control this.
Speculating what this could mean...
Speculating what this could mean...
4/ Trump’s case is more than just mild, or he is receiving steroids when he technically should not be.
Either way, if in fact his symptoms started on Thursday, then the next several days will be very important to watch closely.
Either way, if in fact his symptoms started on Thursday, then the next several days will be very important to watch closely.
• • •
Missing some Tweet in this thread? You can try to
force a refresh


