Brilliant presentation by Dr. @PPibarot on Aortic Valve Calcium Score @MonteHeart CT/CMR Lecture on 10/16/20.
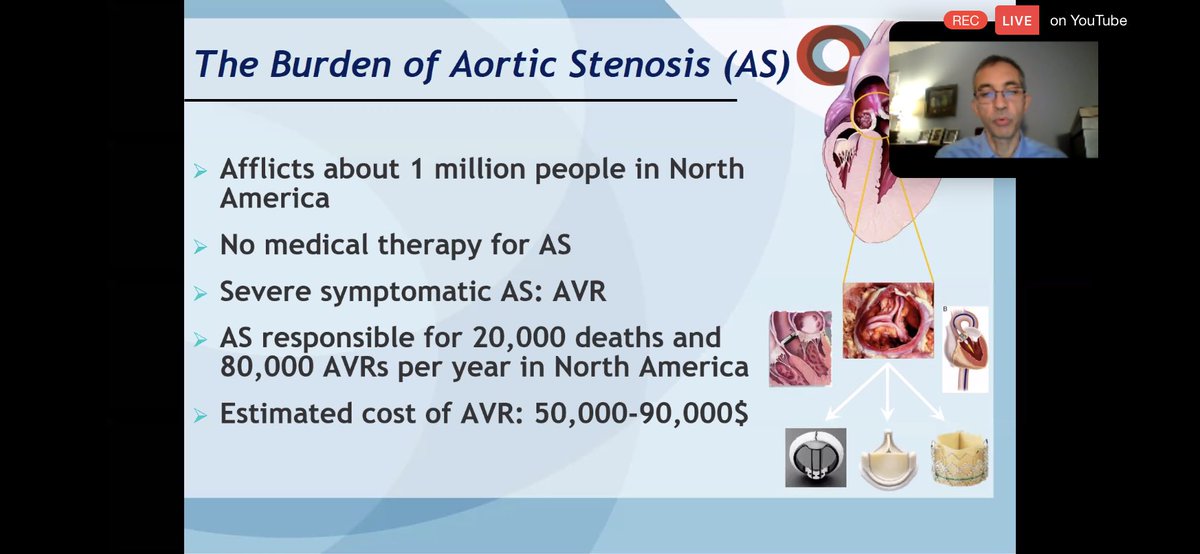
💥Important to begin by appreciating burden of AS.
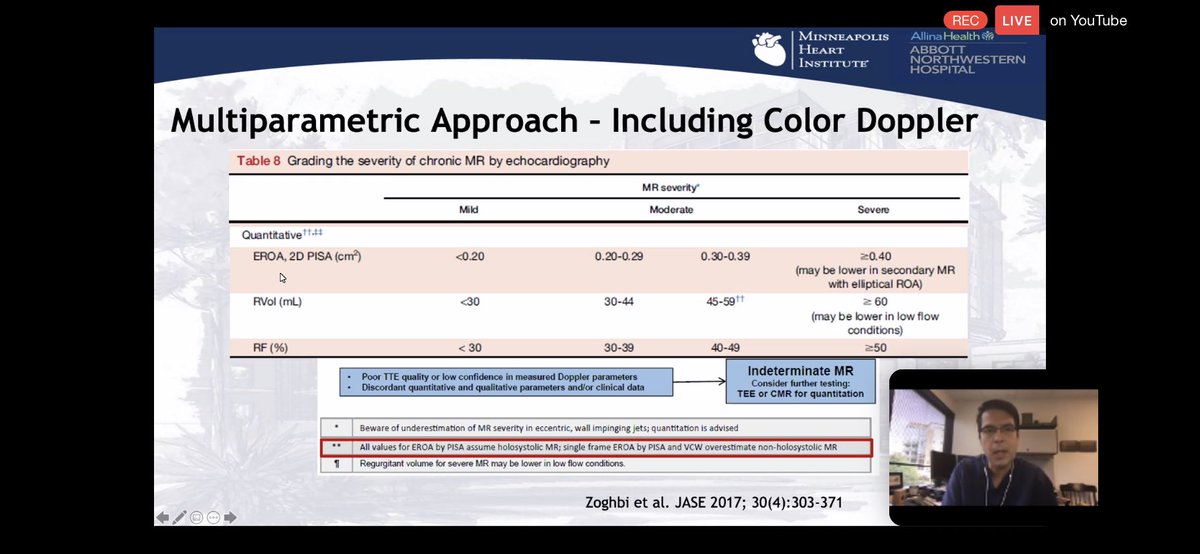
💥#echofirst remains primary modality to assess HEMODYNAMIC severity.
💥Need other tools to assess ANATOMIC severity!
💥Important to begin by appreciating burden of AS.
💥#echofirst remains primary modality to assess HEMODYNAMIC severity.
💥Need other tools to assess ANATOMIC severity!


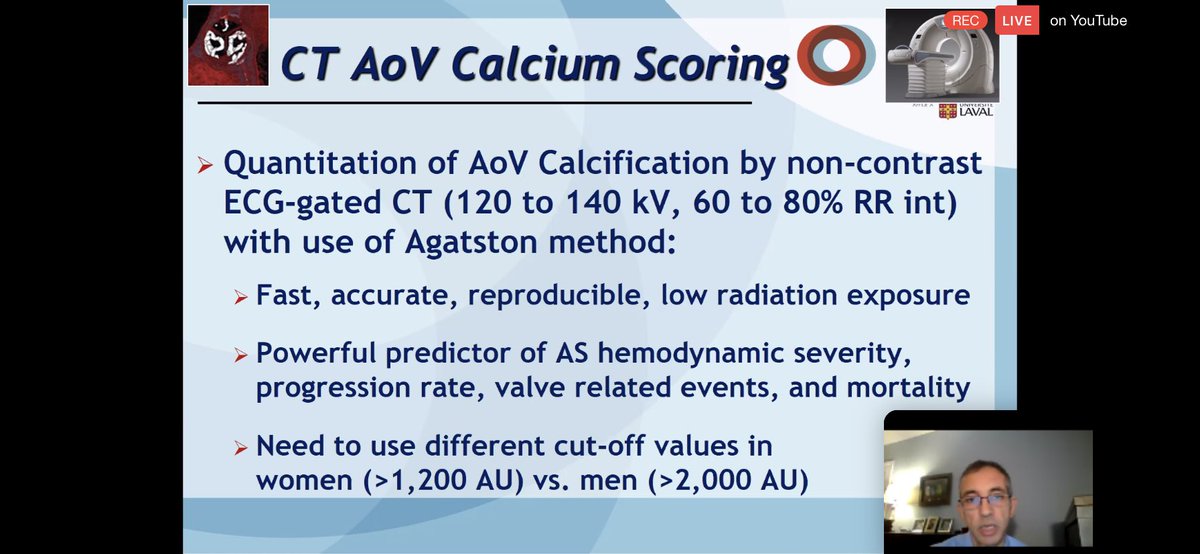
💥JACC 2019➡️Review non-contrast CT to measure AVC in AS.
💥An example protocol by Dr. @PPibarot ⬇️ measuring calcium burden in en-face view of AV.
💥Pitfalls: inclusion of LVOT, sorta, mitral annulus & cors. Multi-planar reconstruction helps carefully exclude non-AV calcium.
💥An example protocol by Dr. @PPibarot ⬇️ measuring calcium burden in en-face view of AV.
💥Pitfalls: inclusion of LVOT, sorta, mitral annulus & cors. Multi-planar reconstruction helps carefully exclude non-AV calcium.




💥Women & Men are different! For a given amount of AVC, 🚺 have a ⬆️ peak jet vel. by #echofirst. For a given peak vel. by #echofirst 🚹 have higher iAVC.
💥AVCd didn’t help resolve the discordance.
💥2017 ESC guidelines for severe AVC ➡️>1200 AU 🚺,>2000AU🚹.
💥AVCd didn’t help resolve the discordance.
💥2017 ESC guidelines for severe AVC ➡️>1200 AU 🚺,>2000AU🚹.



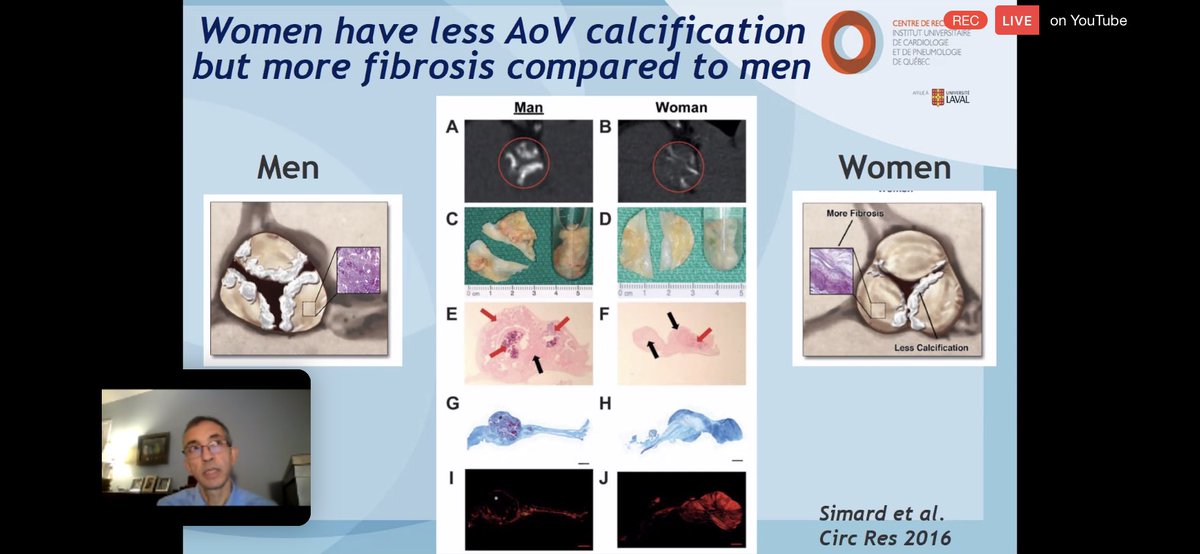
💥Reason for sex disparity was recognized as being ⬆️ fibrosis in 🚺 compared to 🚹
💥In young patients w/ bicuspid AV(YBAV) ⬆️HEMODYNAMIC severity of AS was found in absence of significant AVC.
💥YBAV usually identified by #echofirst alone.Older pts w/ LFLG benefit from #yescct
💥In young patients w/ bicuspid AV(YBAV) ⬆️HEMODYNAMIC severity of AS was found in absence of significant AVC.
💥YBAV usually identified by #echofirst alone.Older pts w/ LFLG benefit from #yescct


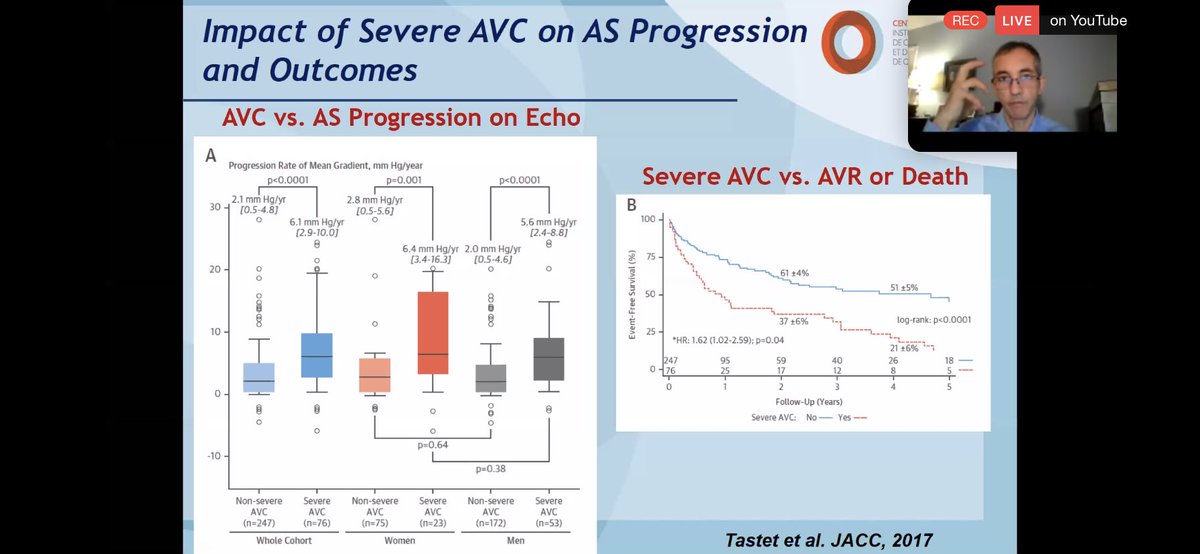
💥But does our knowledge of ANATOMIC severity of AVC w/ #yesCCT impact outcomes?
💥YES ⬇️ severe AVC at baseline predicts outcome (survival) as well as rate of progression.
💥YES ⬇️ severe AVC at baseline predicts outcome (survival) as well as rate of progression.


💥Moving on to using #yesCCT AVC as a tie-breaker in low-gradient AS. Beautifully outlined below.


💥Future perspectives 1
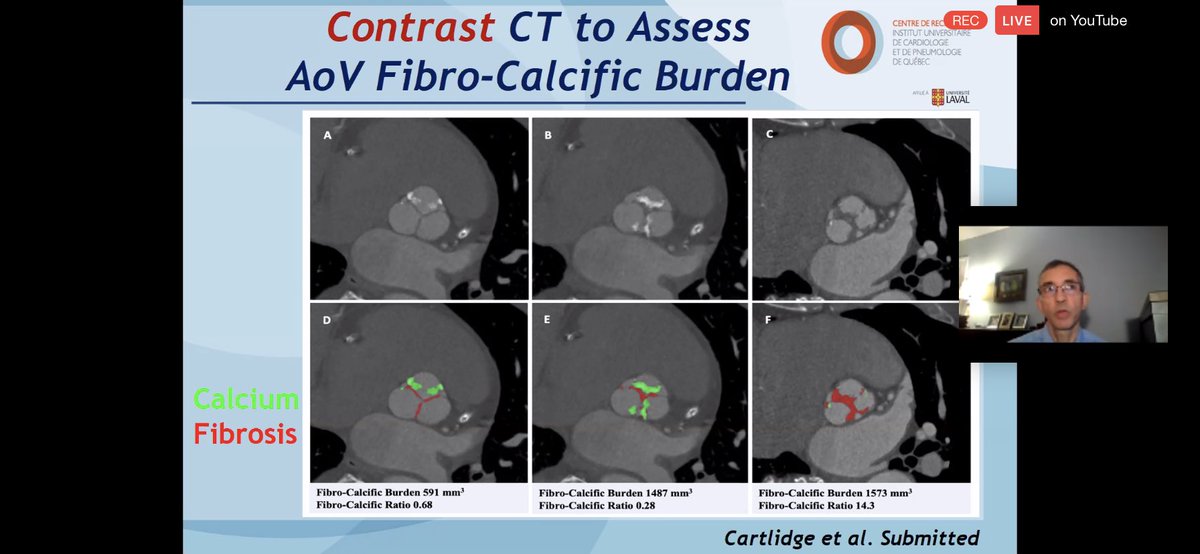
💥Contrast #yescct to assess AV fibro-calcific burden (FCB). Might be particularly useful in 🚺.
💥example: 3 cases with similar #echofirst. Calcification=3SD above mean attenuation in blood pool,rest= fibrous tissue.
💥FCB ⬆️⬆️ with severe AS & in 🚺.
💥Contrast #yescct to assess AV fibro-calcific burden (FCB). Might be particularly useful in 🚺.
💥example: 3 cases with similar #echofirst. Calcification=3SD above mean attenuation in blood pool,rest= fibrous tissue.
💥FCB ⬆️⬆️ with severe AS & in 🚺.



💥Future perspectives 2
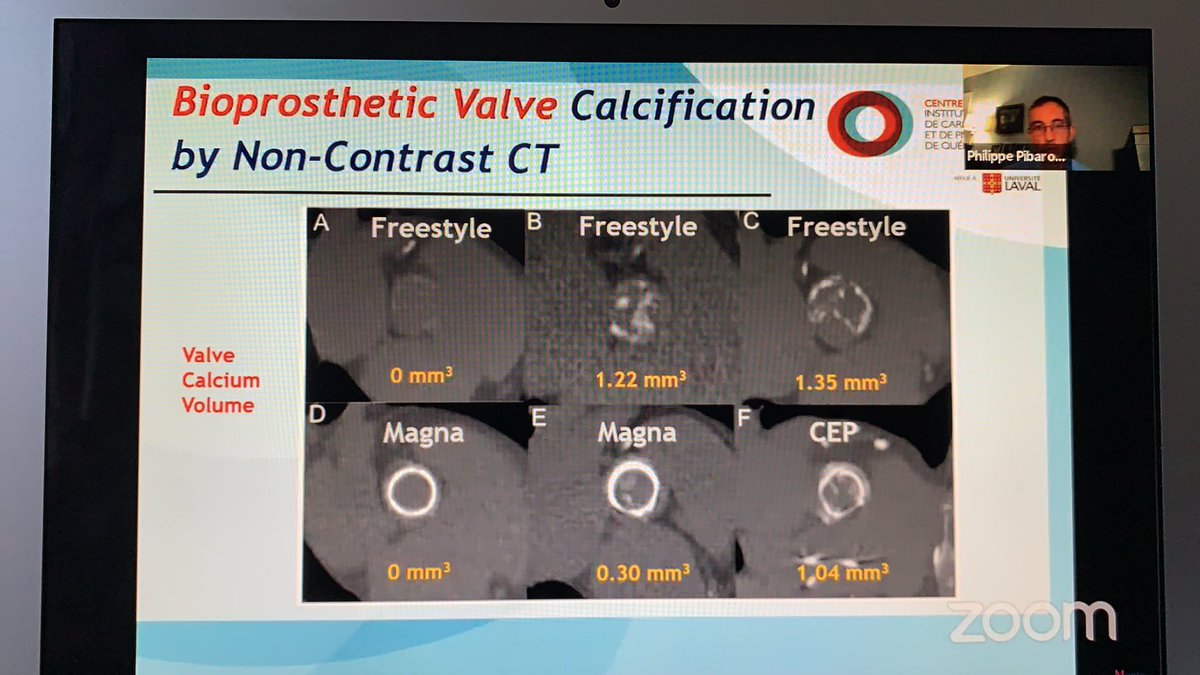
💥Use of non-con #yesCCT to assess bAV calcification aka structural valve deterioration (SVD) using the poly metric method.
💥isolates SVD by #yescct aka early stage a/w 2-fold ⬆️d risk of 💀 or re-intervention.
💥Use of non-con #yesCCT to assess bAV calcification aka structural valve deterioration (SVD) using the poly metric method.
💥isolates SVD by #yescct aka early stage a/w 2-fold ⬆️d risk of 💀 or re-intervention.

💥Future perspectives 3
💥Using NaF PET-CT to identify microcalcification and predict disease progression.
💥Using NaF PET-CT to identify microcalcification and predict disease progression.

💥Concluding this incredible talk⬇️
💥🎥 with QA session can be found on @MonteHeart @YouTube channel➡️ youtube.com/channel/UCY8Wj….
💥🎥 with QA session can be found on @MonteHeart @YouTube channel➡️ youtube.com/channel/UCY8Wj….

• • •
Missing some Tweet in this thread? You can try to
force a refresh