Just finished watching the fantastic #IDWeek2020 session “Top Papers in Medical Mycology” by Drs. Jeniel Nett and @petergpappas, highly recommend watching. They covered notable papers, and I took a stab at high-level summaries with screenshots below. @MSG_ERC @IDSAInfo @SIDPharm
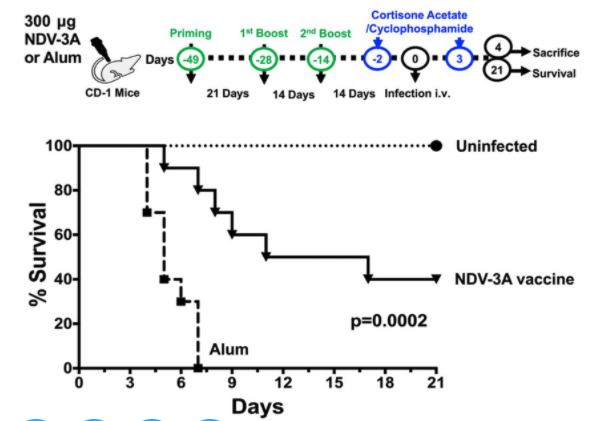
1) 10.1371/journal.ppat.1007460 – NDV-3A Vaccine protects mice against MDR-C. auris infection; N-terminus of Als3 protein (major adhesion/invasin from C. alb) formulated with alum; Anti-Als3 Abs in mice recognized C. auris in vitro, blocked biofilm/enhanced macrophage killing. 
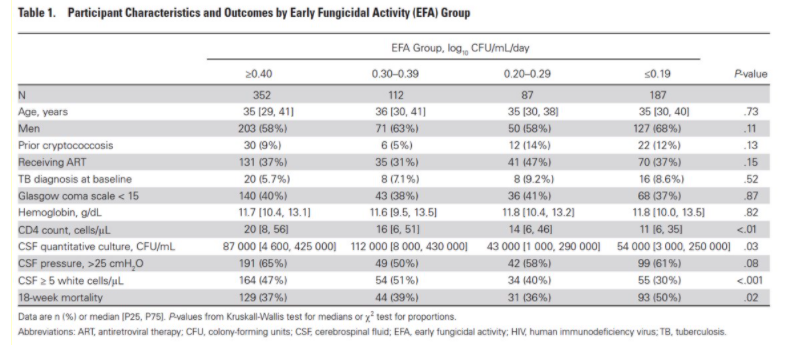
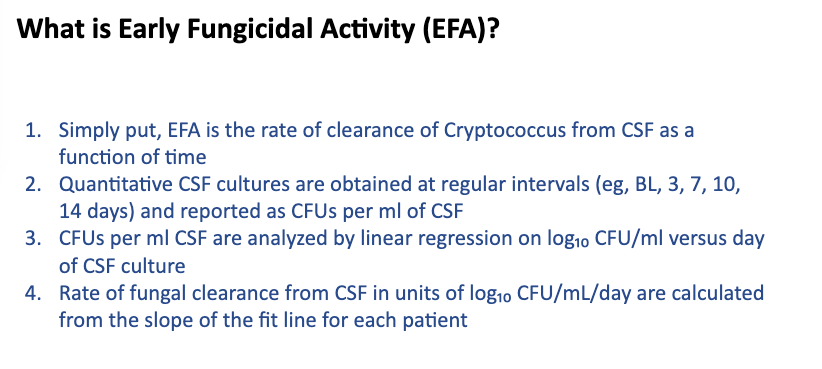
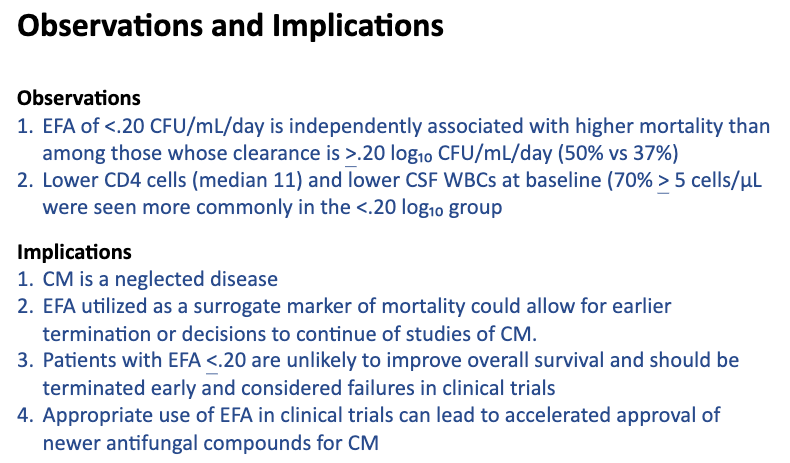
2) 10.1093/cid/ciaa016 – CSF early fungicidal activity as surrogate endpoint for Crypto mening. survival in trials. 738 pts w/ CM & serial LPs; EFA (pic1) measured thru d10 and pts with low EFA had sig. higher 18-wk mortality compared to higher EFA, also low EFA pts ~ low CD4s.
3a) 10.1038/s41586-019-1608-2 – Fungal mycobiome -> panc oncogenesis via mann binding lectin; Mycobiota expansion a/w panc ductal adeno CA; Despite expansion in burden, decreased diversity w/ inc Malassezia (20% pop.); AmB admin led to several anti-onc changes (pic 2).
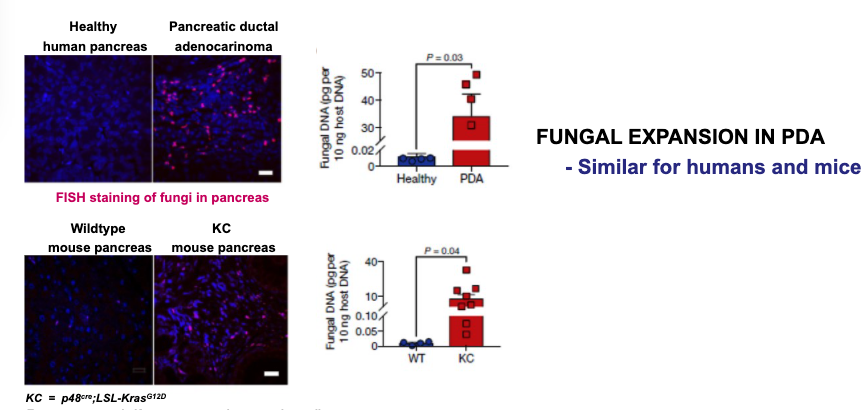
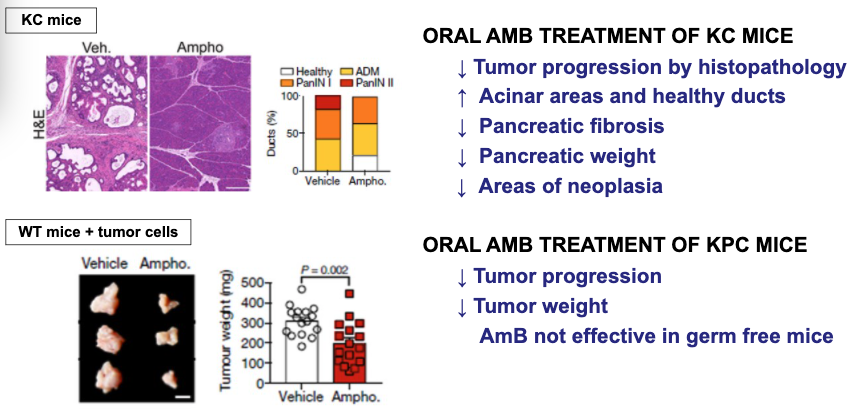
3b) Rechallenge w/ Malassezia -> inc tum wt/progression, but similar not shown for Aspergillus/Candida/Saccharo. Mannose binding lectin might be culpable -> fung recognition/complement activation/tum growth. Expression a/w dec surv in database pts. MBL disruption ~ inc survival.
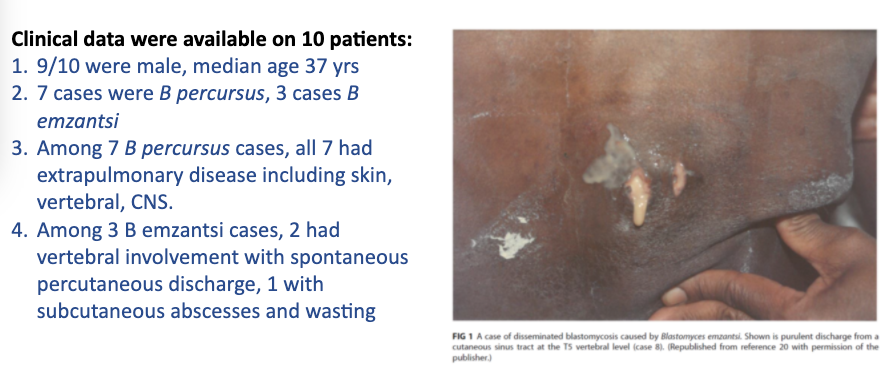
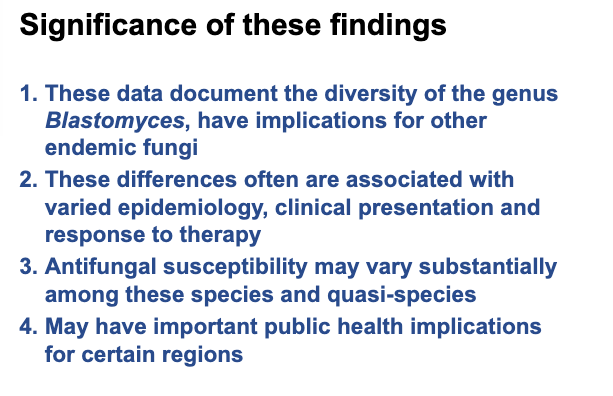
4) 10.1128/JCM.01661-19 – Blastomycosis in S. Africa by B. percursus/emzantsi 1967-2014; Review of 20 “B. dermatiditis” cases; Clinical data (pic 1), all w/ extra-pulm dz, higher than expect for B. derm. Sequencing revealed B. percursus/emzantsi, significance (pic 2)
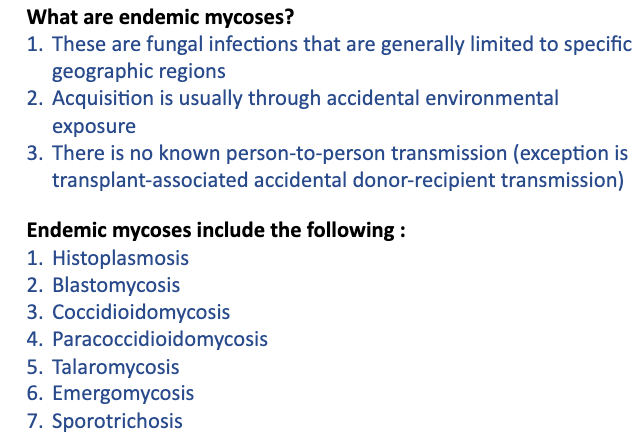
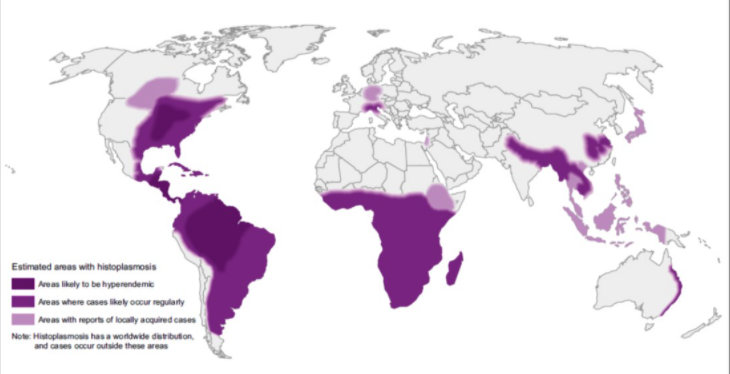
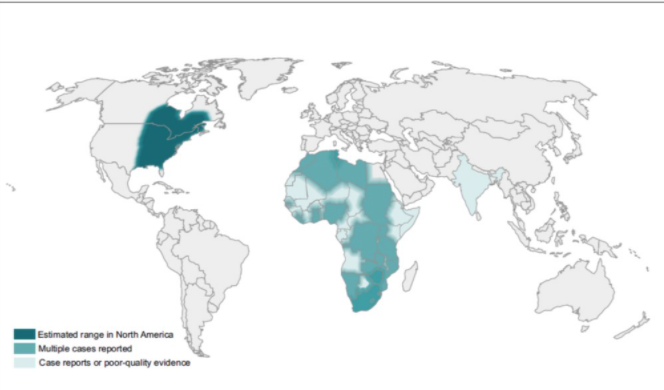
5) 10.1007/s11046-020-00431-2 – Redrawing endemic mycoses map; list of endemic mycoses (pic 1); Histo (pic 2), Blasto (pic 3) Coccy (pic 4). Summary, maps are changing with better reporting/improved diagnostics, climate change, migration/travel.

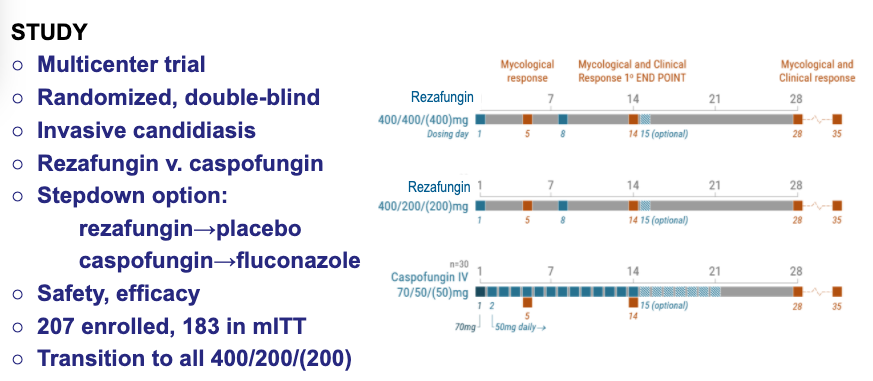
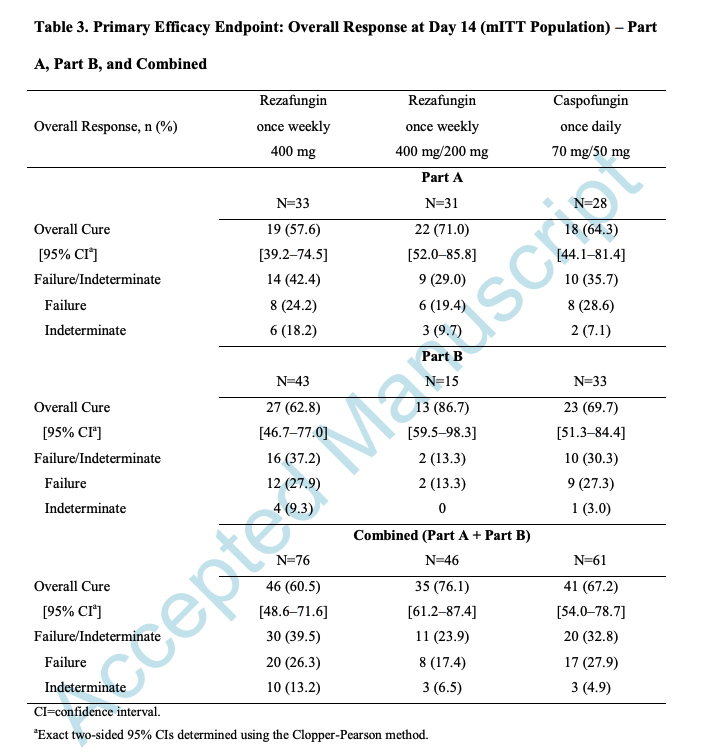
6) 10.1093/cid/ciaa1380 – STRIVE reza vs. capso for candidemia/candidiasis; Design (pic 1) two reza arms vs caspo w/ step-down fluc; High dose reza (400/wk) stopped after review unblinded early data; Overall cure d14 similar among groups (pic 2), no concerning safety trends.
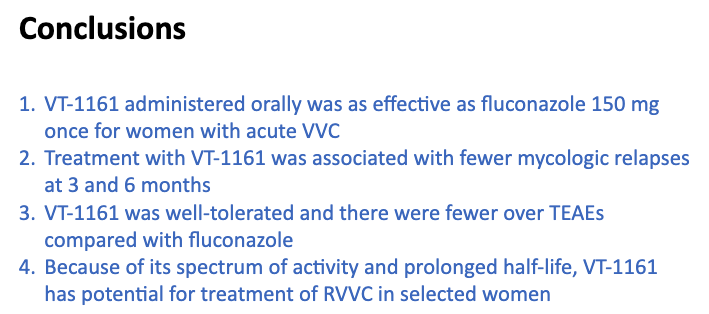
7) 10.1093/cid/ciaa1204 – Phase 2 VT-1161 (oteseconazole) for acute VVC; Novelty in VT-1161 = higher specificity fungal CYP51, half-life >60 DAYS; Dose-finding (3 regimens) vs. fluc 150 x1 (Small n = 55), similar response rate, lower Cx (+) relapse w/ VT. Conclusions (pic1).
8) 10.1093/infdis/jiaa394 – Core recs for antifungal stewardship by @msgerc; 7 core ASP elements specific to antifungals (1 leadership 2 accountability 3 expertise 4 education 5 ID C/s & bundles (pic 1), audits 6 surveillance 7 reporting/feedback; Encourage reading.
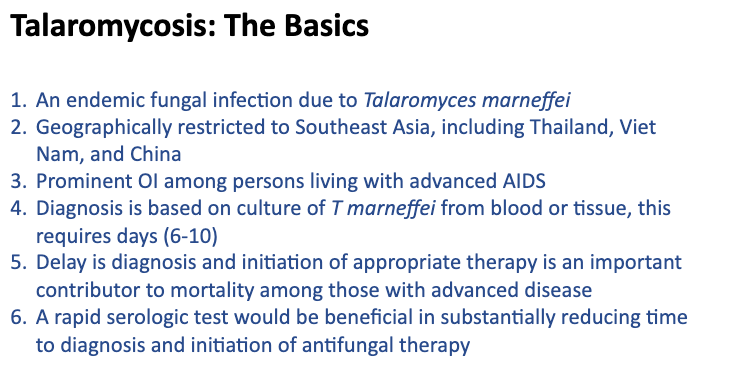
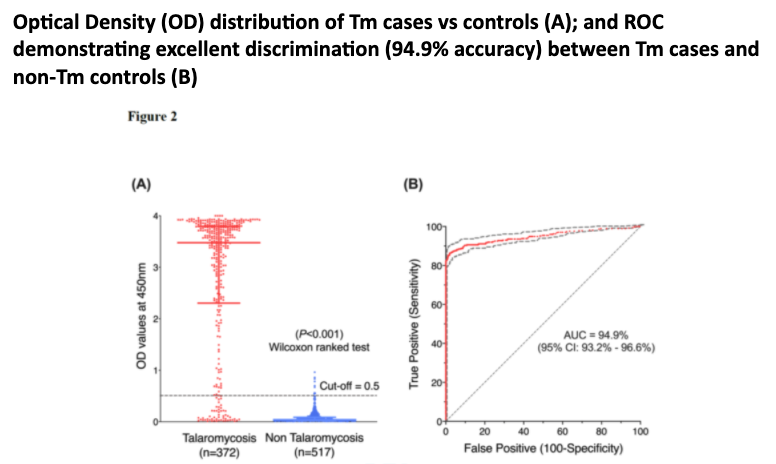
9) 10.1093/cid/ciaa826 –Superiority of Mp1p antigen EIA vs BACTEC bcx for dx of talaromycosis; The basics (pic 1), delay in dx/tx problematic. Samples from Cx + pts used. No Ag x-reactivity w/ other fungs. ROC curve (pic 2), superior to BCx, urine/serum can be used, ~6d quicker.
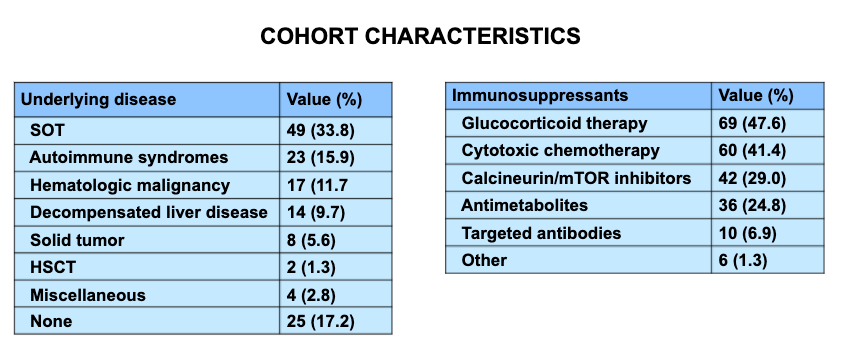
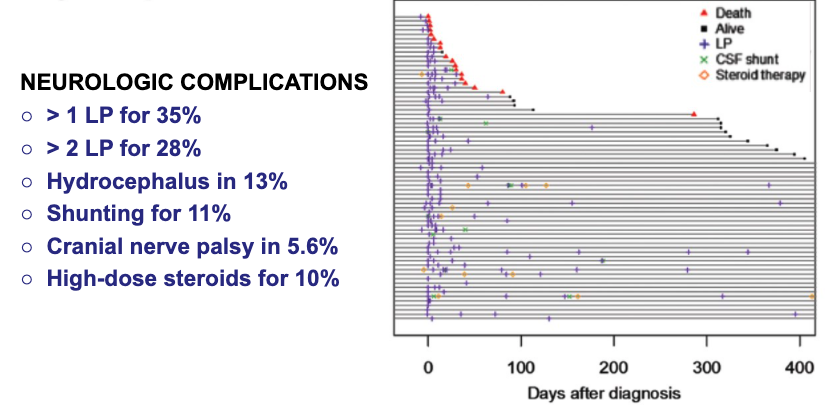
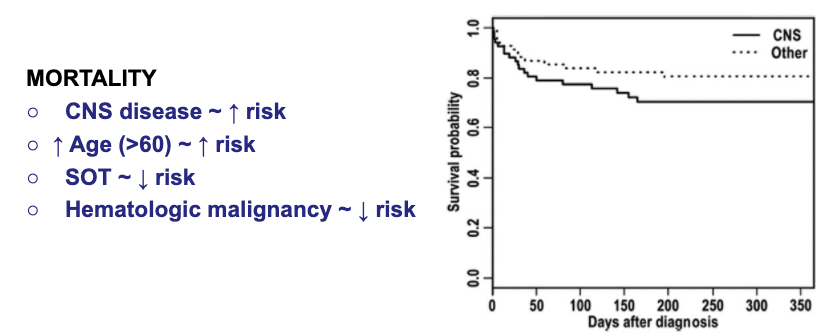
10) 10.1093/cid/ciz193 – Longitudinal non-HIV cryptococcosis in US n=145,CNS=71, 2/3 proven,1/3 prob; Characteristics (pic1),presentation – most w/o fever, neurologic/pulm sx varied by site; CrAg higher in CNS, delayed dx common, neuro complications (pic2), mortality (pic3).
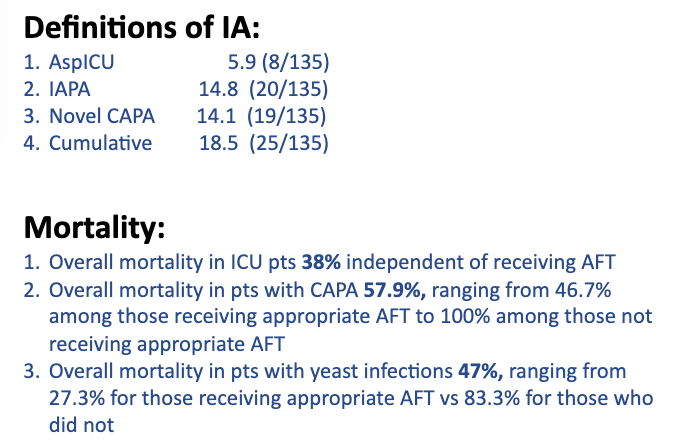
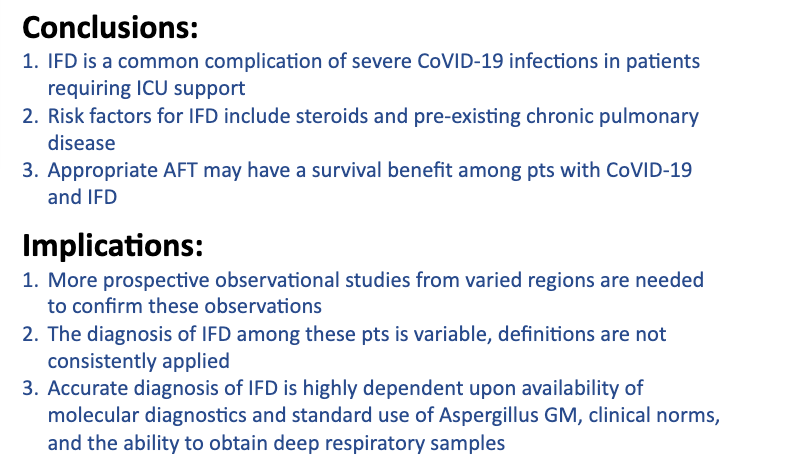
11a) 10.1093/cid/ciaa1298 – National strategy for CAPA Diagnosis in ICU; Prospective cohort, SOC = serum/BAL GM, Asp PCR, B-Dgluc, blood/deep resp Cx; Tx per discretion of MD. Among 135 screened, 51 (37%) ±1 pos mycologic test (30 Asp); Sig RF = high-dose ster, underlyin resp dz;
11b) Varying degree of IA by definition (pic 1), mortality sig higher in pts classified as having IFD, CAPA 57.9% (lower w/ approp tx), yeast infxns 47% (lower w/ approp tx). Conclusions (pic 2), need more prosp. data, accurate dx requires consistently applied definition.
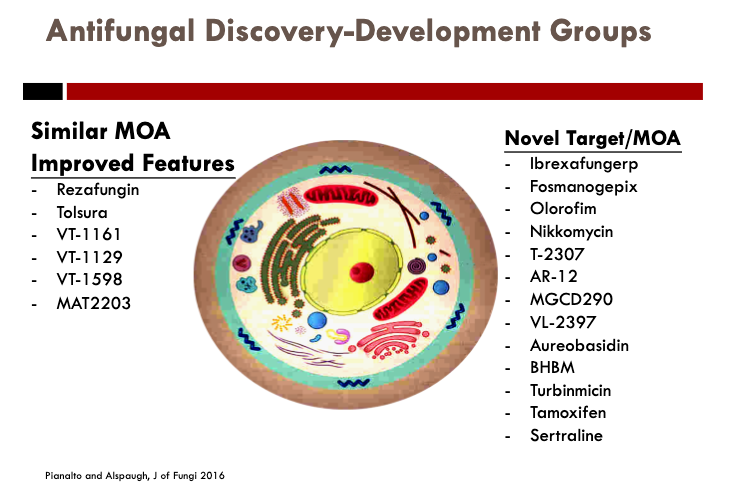
Concluding remarks: It is a very exciting time in medical mycology and antifungal therapeutics! The antifungal pipeline is promising (fosmano, olorfim, ibrexafungerp, VT-1161, reza, oral ampho, etc.). Stay tuned! @IDSAInfo @SIDPharm @MSG_ERC @FungalDoc @GermHunterMD @ErinMcCreary
• • •
Missing some Tweet in this thread? You can try to
force a refresh