
On the multiple vaccine problem...
@Dereklowe argues that 1st EUA for a COVID vaccine will make it hard to recruit for other vaccine trials. @ht @tylercowen
There's a solution: PAY PARTICIPANTS TO ENROLL. (Thread.) @arpitrage
'The Vaccine Tightrope blogs.sciencemag.org/pipeline/archi…
@Dereklowe argues that 1st EUA for a COVID vaccine will make it hard to recruit for other vaccine trials. @ht @tylercowen
There's a solution: PAY PARTICIPANTS TO ENROLL. (Thread.) @arpitrage
'The Vaccine Tightrope blogs.sciencemag.org/pipeline/archi…
I modeled & argued this in the 2019 J Human Capital paper below & a 2011 @nberpubs working paper (both w T Philipson).
journals.uchicago.edu/doi/abs/10.108…
nber.org/papers/w17011#…
journals.uchicago.edu/doi/abs/10.108…
nber.org/papers/w17011#…
@ATabarrok makes this point & offers more options on Marginal Revolution. marginalrevolution.com/marginalrevolu…
Can Medical Progress be Sustained? Implications of the Link Between Development and Output Markets
Can Medical Progress be Sustained? Implications of the Link Between Development and Output Markets
The problem--not just for the COVID vaccine but also all drugs--is that bioethical rules capping payment for participation limit the supply of volunteers, esp for placebo-controlled trials. Econ 101 tells you this is inefficient. @jonathangruber1 @Noahpinion @C_Garthwaite
But let's get the bioethics out of the way first. 1/If you're consequentialist, it's easier to get to this conclusion. (I know very few ppl who aren't even partly consequentialist.) @CohenProf @PetrieFlom @MichelleM_Mello @HollyLynchez
2/Let's deal w the deontological objections. a/If you believe inconsistency, then opposing payment for trial participants requires you to oppose paying health care workers/soldiers/construction workers who risk their lives for the risk they face at work.
b/One riposte is that payment is coercive, esp for the poor. But that implies wages for those other jobs are coercive too. Why don't these ppl oppose those? Or, we can have more robust informed consent for taking those jobs or requiring it for entering trials.
Aside: if you believe in autonomy or info asymmetry (ie we may now know what poor actually think), then the argument against paying trial subjects is even harder. I also think it's a bad posture for intellectuals to tell poor ppl what they can & cannot do for work.
c/Another arg against trial wages is abhorrent markets: ppl don't want ppl to pay for body parts. I worry the problem is just that opponents don't want to know abt it. HCW/soldiers/etc. are already paid for those risks. Opponents pay for those, w/o vocal objection.
Also, more specifically, we do pay for body parts already. Trial participants are partly compensated now; that's included in drug costs. (We're talking about paying more.) We do pay for blood donations, hair.
Given all this, it is unsurprising that bioethicists are shifting their stance. E.g., @ZekeEmanuel:
journals.sagepub.com/doi/10.1111/j.…
journals.sagepub.com/doi/10.1111/j.…
Back to consequentialism. Let's look at redistribution. If you care about the poor, wages will benefit the poor in a net present value sense. If you have trial wages, drugs are developed faster, so they become generic faster and thus affordable to the poor faster.
(BTW, if you are a cosmopolitan and you care about redistribution, you should be even more concerned. An alternative to recruiting more in the US is conducting foreign trials in poor countries.)
I could go on, but let's return to economics. The problem is basic: trial participants are workers who contribute effort & their bodies to help produce info abt drugs. If you cap wages, drug producers have to search longer to find enuf people to meet sample size requirements.
That delays drugs. The delay harms consumers. You could solve the problem by lowering the sample size requirement or approving w/ less info abt drugs (but perhaps with ex post tort protections). TBH, I don't know the full value of 95% confidence in efficacy or safety.
But if you want the info & fast, then you have to pay. What makes this market complicated is exactly what @Dereklowe points out: approving 1 drug makes it hard to get a 2nd drug in the same class approved because participants.
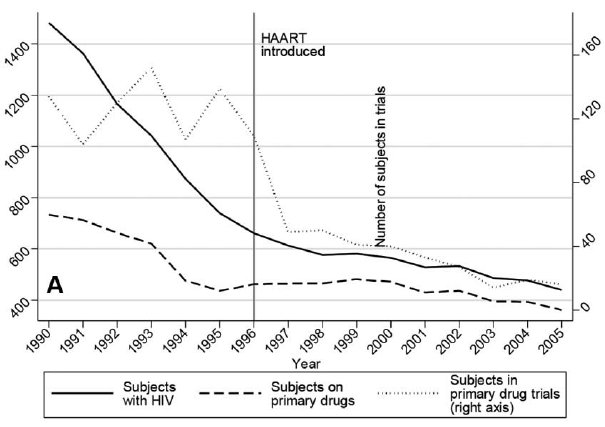
Our 2019 paper showed that when HAART (for AIDs) was approved, trial participation (in a panel dataset on homosexual males) fell (dotted line) dramatically. Effect was most severe in placebo controlled trials. Number of trials (relative to funding) fell. 
If you think the wages are too high or can't be calculated, think again. Consider a trial w equal chance of getting placebo or a vaccine w expected 70% effectiveness. Outside option is 100% chance of approved vaccine with eg 80% effectiveness. Assume risk from COVID is worth H.
Then crudely the required wage is w = (0.8 - [0.5*0.7]) H = 0.45 H.
What is H? Depends on where you are. But if we just include mortality risk you take the product of i/risk of getting COVID during the duration of the trial, eg, 10%, ii/the mortality risk & iii/value SL.
What is H? Depends on where you are. But if we just include mortality risk you take the product of i/risk of getting COVID during the duration of the trial, eg, 10%, ii/the mortality risk & iii/value SL.
If VSL = 10m,& IFR = 1%, then w = 0.1*10m*0.01 = $10k. (An underestimate because it doesn't include morbidity, but surely < $20k.) Either way, not a crazy amount. This simple exercise reveals a lot of things about trial economics.
-Human challenge trials are more expensive because probability of infection under the trial is greater.
-It's cheaper to do trials abroad bec VSL is lower.
-It's cheaper to do trials on the young bec their risk of death is lower, holding VSL constant.
-It's cheaper to do trials abroad bec VSL is lower.
-It's cheaper to do trials on the young bec their risk of death is lower, holding VSL constant.
-QALYs may be a better approach than VSLs for determining wages. VSL good for govt allocation where we want to assume all lives are worth the same. But in voluntary markets ppl have different VSLs. Holding wealth constant, young value life more bec they have more life years left.
The old value each life year more they have more wealth. The poor value life less because they have less wealth. Liquidity constraints lower demand for the poor & young.
-YOU DON'T HAVE TO GET THE WAGE RIGHT ON THE FIRST TRY. If it's too low, raise it to get faster enrollment.
-YOU DON'T HAVE TO GET THE WAGE RIGHT ON THE FIRST TRY. If it's too low, raise it to get faster enrollment.
Perhaps a positive side effect of COVID is we'll revisit the ethics of paying trial subjects for all drugs. It could hasten all medical innovation. Folks like @Cutler_econ, K Murphy, B Topel & others have argued has great value. (My work w @JulianReif on this in next tweet.)
The insurance value of medical innovation sciencedirect.com/science/articl…
• • •
Missing some Tweet in this thread? You can try to
force a refresh


